|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
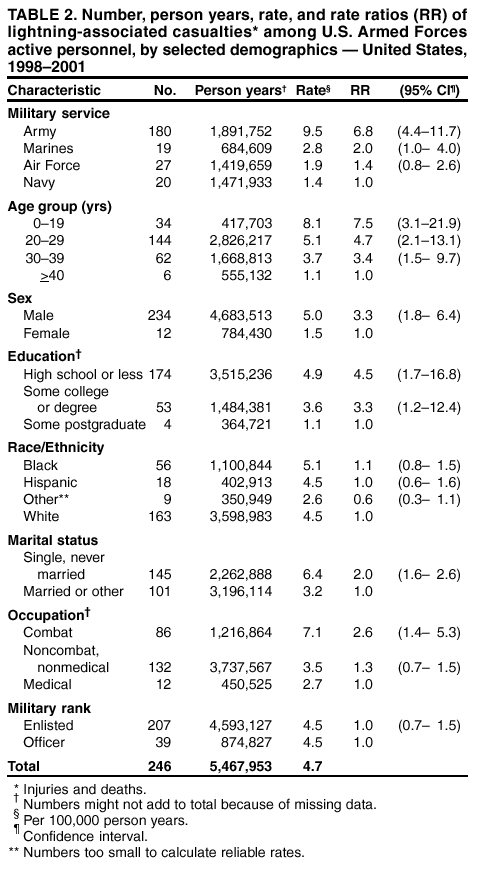
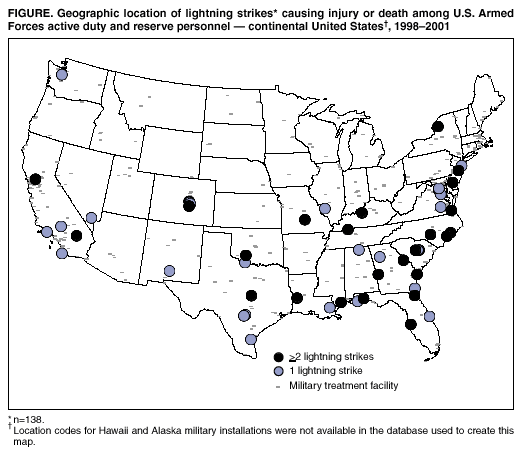
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Lightning-Associated Injuries and Deaths Among Military Personnel --- United States, 1998--2001After flooding, lightning is the second leading cause of weather-related death in the United States; approximately 300 injuries and 100 deaths are associated annually with lightning strikes in the United States (1--4). To characterize lightning-associated injuries and deaths among U.S. Armed Forces personnel, the U.S. Army and CDC analyzed data from the Defense Medical Surveillance System (DMSS). This report summarizes the results of that analysis, which indicate that the highest lightning-related injury rates during 1998--2001 occurred among male U.S. military members who were aged <40 years, single, with a high school education or less, stationed near the Gulf of Mexico or the East Coast, and in the U.S. Army. The findings suggest that the risk for lightning-associated injury depends primarily on the frequency, timing, duration, and nature of outdoor exposure to thunderstorms. Military personnel should be aware of severe weather onset and take reasonable precautions to protect themselves and their companions from exposure to lightning. DMSS maintains hospitalization and ambulatory clinic visit data on U.S. Armed Forces personnel (both active-duty and reserve) and links health data with personnel data (e.g., age, race, sex, education, occupational specialty, and duty station). This analysis considered lightning-associated injuries or deaths among active-duty and reserve military personnel that occurred during 1998--2001. A lightning-associated injury or death was defined as a hospitalization or ambulatory clinic visit in the 50 states and the District of Columbia that was assigned a primary or secondary diagnosis of "effects from lightning, shock from lightning, or struck by lightning" according to the International Classification of Diseases, Ninth Clinical Modification (ICD-9-CM) code 994.0. Because isolated cloud-to-ground lightning strikes could not be distinguished from multiple lightning strikes at the same time and location, it was assumed that two or more lightning-associated injuries or deaths at the same time and location were caused by a single lightning strike. Descriptive statistics were analyzed, including event date, location, percentage of strikes causing injury resulting in hospitalization or death, casualties per strike, and military status (i.e., active or reserve) of affected persons. Because accurate denominator data were not available for reserve personnel, lightning casualty rates and relations of selected demographic factors to those rates were calculated for active-duty personnel only. Military personnel comprise a highly mobile population, and many duty assignments last for <1 year; therefore, lightning-associated casualty rates were expressed as casualties per 100,000 person years. Rate ratios and 95% confidence intervals (CIs) were based on Poisson regression. The descriptive nature of this report precluded calculating adjusted estimates. During 1998--2001, a total of 142 lightning strikes caused 350 service member injuries and one service member death at U.S. military installations in the United States (Figure); 64 (18.0%) persons required hospitalization. The majority (123 [86.6%]) of lightning strikes injured either one or two persons; 12 (8.5%) strikes injured three to nine persons; and seven (4.9%) strikes injured >10 persons, including one that injured 44 persons during an outdoor training exercise. Three fourths (106 [74.6%]) of lightning strikes occurred during May--September, with a peak (71 [50.0%]) during July--August. Lightning strikes occurred more often near the coasts, particularly in southern and eastern areas. Active-duty personnel constituted the majority (246 [70.1%]) of lightning-associated casualties. Overall, the lightning strike casualty rate was 5.8 per 100,000 person years (Table 1). By state, Louisiana (39.6), Georgia (25.2), and Oklahoma (23.5) had the highest rates. Comparisons among age groups showed a strong inverse relation between age and risk for lightning-associated injury (Table 2). Men were 3.3 times more likely than women to be struck by lightning. Service members with a high school education or less and those in combat-related occupations (e.g., infantry or artillery) were at higher risk than their counterparts. Among the services, the Army had the highest lightning casualty rate (9.5), and the Navy had the lowest (1.4); the Army-to-Navy rate ratio was 7.0 (95% CI=4.4--11.7). Reported by: MJ Silverberg, PhD, A Frommelt, MPH, JL Lange, PhD, JF Brundage, MD, MV Rubertone, MD, BH Jones, MD, Army Medical Surveillance Activity, US Army Center for Health Promotion and Preventive Medicine. BS Winterton, DVM, EIS Officer, CDC. Editorial Note:The findings in this report are consistent with previous studies indicating that the majority of lightning-associated casualties were men aged <40 years (2). However, among military personnel, this age and sex distribution reflects the overall make-up of the military and also might reflect age and sex differences in military occupational or recreational exposure to lightning hazards. Previous studies found that the highest lightning-associated mortality frequencies were reported in Florida and Texas (2,3) and the highest lightning-associated mortality rates were in Arizona, Arkansas, Florida, Mississippi, New Mexico, and Wyoming (1,3). The difference in geographic distribution of lightning casualties between those reported here and those reported previously reflects the geographic distribution of military service members across the United States; a disproportionate number of service members are stationed in rural areas and in southern and eastern coastal states. Service members in combat occupations (generally associated with increased outdoor exposure) had higher casualty rates than those in other military occupations. These findings suggest that lightning injury risk is determined by the frequency, timing, duration, and nature of outdoor exposure to thunderstorms and that specific demographic factors (age, sex, education, and race) are associated with lightning injury risk only to the extent they correlate with the primary risk determinant. Lightning-associated injuries and deaths among military personnel might be undercounted for at least three reasons. First, because casualties were determined from military inpatient and outpatient records at "fixed" U.S. military medical treatment facilities, military casualties treated at deployed or "field" military medical treatment facilities might not be represented fully. Second, because external cause-of-injury codes ("E codes," including ICD-9-CM code E907) are not used in the Military Health System, any lightning-associated casualties assigned codes other than ICD-9-CM code 994.0 would not have been captured. Finally, deaths not preceded by hospitalization or ambulatory clinic visit could not be ascertained. Approximately 30 million cloud-to-ground lightning strikes occur each year in the United States (5), each of which has the potential to cause serious injury and death. U.S. military personnel are a potentially high-risk population for lightning-associated injury and death because military training and operational activities occur outdoors in all types of weather conditions and within areas of the country with high lightning-associated morbidity and mortality. The identification of features common to lightning strike victims can be used to focus prevention efforts. Persons with outdoor exposure during active military service should be aware of approaching severe weather and should take reasonable precautions to protect themselves and their fellow soldiers, sailors, airmen, and marines. Guidelines for preventing lightning-related injuries are available from the National Lightning Safety Institute at http://www.lightningsafety.com/nlsi_pls/1st.html. These guidelines are equally applicable to military personnel and to anyone else with potential exposure to thunderstorms. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 9/26/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 9/26/2002