 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Usual Sources of Cigarettes for Middle and High School Students --- Texas, 1998--1999Persons often begin smoking when they are minors (aged <18 years) (1,2), and easy access to cigarettes might contribute to this behavior (3). Laws and regulations were in place in Texas during 1998--1999 to reduce minors' access to cigarettes by 1) prohibiting the sale and distribution of tobacco products to minors; 2) imposing fines against retailers caught selling cigarettes to minors; 3) prohibiting minors from purchasing, possessing, or using tobacco products; 4) limiting vending machines to adult-only locations; and 5) requiring tobacco retailers to ask for proof of identification from anyone attempting to purchase tobacco who appeared to be aged <27 years (4). To measure progress in reducing access to cigarettes among middle and high school students in Texas, CDC analyzed self-reported data from the 1998 and 1999 Texas Youth Tobacco Survey (TYTS). This report summarizes the results of that survey, which indicate that during 1998--1999, reported access to cigarettes from stores and vending machines (commercial sources) decreased among middle school students from 13.2% to 5.3% and from 7.6% to 1.7%, respectively, but access from noncommercial and other sources (e.g., stealing cigarettes and "getting them some other way") increased from 8.3% to 12.3% and from 16.6% to 23.3%, respectively. Among high school students, most sources did not change. Educating retailers and actively enforcing laws governing youth access to tobacco as part of a comprehensive tobacco-control approach are required to reduce youth access to cigarettes. The Texas Department of Health conducted the statewide TYTS in spring 1998 and spring 1999. TYTS uses a two-stage cluster sample design to produce representative samples of public middle and high school students in Texas. The first-stage sampling included all public schools containing any grades 6--12. The probability of a school being selected depended on its enrollment size. A total of 214 schools were sampled in 1998 and 276 in 1999. At the second stage of sampling, second-period classes were selected randomly, and all students in these classes were eligible to participate. The overall response rate* was 71.2% in 1998 and 61.0% in 1999. School participation rates decreased from a combined (middle and high school) response rate of 84.6% in 1998 to 73% for middle schools and 69.1% for high schools in 1999. Students completed an anonymous, self-administered questionnaire that included questions on demographics, cigarette-smoking status, and sources of tobacco products. Students who reported having smoked during the 30 days preceding the survey were asked, "During the past 30 days, how did you usually get your own cigarettes?" Data were weighted to provide estimates that could be generalized to all public school students in grades 6--12 in the state. SUDAAN 7 was used to calculate standard errors for determining 95% confidence intervals (CIs). During 1998--1999, the percentage of middle school students who smoked during the preceding 30 days and who reported buying cigarettes from a store decreased from 13.2% (95% CI=+1.0) to 5.3% (95% CI=+1.0), and the percentage of those who reported buying from vending machines decreased from 7.6% (95% CI=+1.0) to 1.7% (95% CI=+0.4) (Table). A significant increase was reported among those who reported stealing cigarettes (8.3% [95% CI=+0.9] in 1998 and 12.3% [95% CI=+1.9] in 1999) or getting them in "some other way" (16.6% [95% CI=+1.2] in 1998 versus 23.3% [95% CI=+2.4] in 1999). Among high school students, no significant change was observed during 1998--1999 in the percentage who bought cigarettes from a store (33.0% [95% CI=+1.7] in 1998 and 31.1% [95% CI=+1.6] in 1999). A small but statistically significant decrease was observed in the percentage who reported buying cigarettes from vending machines (1.8% [95% CI=+0.4] versus 1.0% [95% CI=+0.3]) in 1999. A small but statistically significant increase also was observed in the percentage who reported that "an older person" gave them cigarettes (8.0% [95% CI=+0.8] in 1998 and 10.5% [95% CI=+1.3] in 1999). Reported by: P Huang, MD, C Alo, MD, D Satterwhite, Texas Dept of Health. R Caraballo, PhD, L Pederson, PhD, Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion; JC Zevallos, MD, EIS Officer, CDC. Editorial Note:The findings in this report document a decrease in access to cigarettes from stores for middle school students in Texas and a decrease in access to cigarettes from vending machines for both middle and high school students. However, the percentages of middle school students who reported stealing cigarettes or getting them "in some other way" increased. The percentage of high school students who reported getting cigarettes from an older person also increased. These findings suggest an increase in the use of alternative sources for acquiring cigarettes (e.g., stealing or getting them from other adolescents, parents, and older friends) (5). The findings in this report are subject to at least three limitations. First, these data apply only to youth who attend public schools in Texas and might not be representative of all persons in this age group. The average dropout rate for Texas middle and high school students during school years 1997--98 and 1998--99 was 16%, and approximately 10% of middle and high school students are enrolled in private schools (6--8). Second, the decline in school participation rates could have affected the validity of the 1998-1999 comparisons if the nonrespondents in 1999 differed from the respondents. However, given the size of some of the changes in access patterns, it is unlikely that the decrease in response rates would account for all of the changes observed. Finally, a substantial proportion of middle school students responded that they obtained tobacco products "in some other way." Future surveys should include an open-ended category to learn how students obtained tobacco products. Studies designed to determine if reducing illegal cigarette sales to minors can reduce youth smoking prevalence suggest that substantial decreases (to as low as 3%) in illegal sales will be needed to decrease youth smoking prevalence (9). In Texas, the illegal sale rate to minors decreased from 24.0% in 1998 to 13.0% in 1999; a reduction in cigarette smoking prevalence for those years among middle school students (20.0% to 14.8%) also was observed, but not among high school students (33.0% and 32.7%, respectively). However, it is impossible to know if the reduction in smoking prevalence among middle school students is linked directly to reductions in self-reported access to cigarettes in stores or from vending machines. To reduce youth access to cigarettes, stricter policies prohibiting the sale of tobacco to minors are needed, and retailer and community education should be intensified. In addition, a comprehensive approach to prevent both minors and adults from using tobacco should include 1) local community programs, 2) evidence-based school programs, 3) tobacco counter marketing, 4) tobacco-use cessation programs, and 5) surveillance and evaluation systems to monitor progress in reducing the use of tobacco (10). References
* Derived by multiplying the number of schools participating divided by the number of schools sampled by the number of completed surveys divided by the total number of students who would have been surveyed if all had participated.
Table 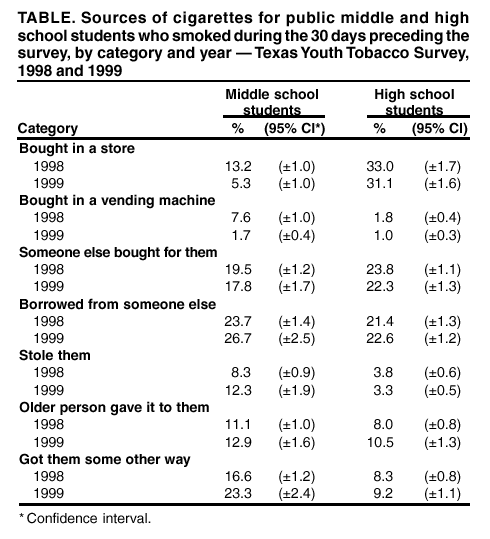 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 10/10/2002 |
|||||||||
This page last reviewed 10/10/2002
|