|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
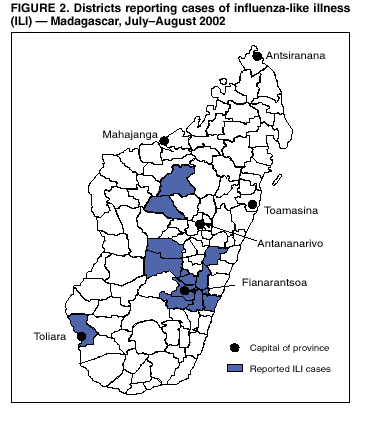
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Influenza Outbreak --- Madagascar, July--August 2002Please note: An erratum has been published for this article. To view the erratum, please click here. In mid-July 2002, Madagascar health authorities were notified of a substantial number of deaths attributed to acute respiratory illness (ARI) in the village of Sahafata (population: 2,160), located in the rural highlands of Fianarantsoa Province, southeastern Madagascar (Figure 1). This region is approximately 450 km (280 miles) south of the capital Antananarivo. The Madagascar Ministry of Health (MOH) and the Institut Pasteur, Madagascar (IPM) initiated an investigation, which found an attack rate of 70% for ARI, with 27 deaths in Sahafata. Pharyngeal swab specimens were collected from ill persons for viral culture. Of the four influenza A viruses that were isolated at IPM, two were identified as type A (H3N2) viruses. In late July, health authorities investigated a similar outbreak in Ikongo District, Fianarantsoa Province. In August, MOH requested assistance from the World Health Organization (WHO) and CDC in investigating the outbreak. In response, an international team of experts from CDC; Institut de Veille Sanitaire, France; Institut Pasteur, France; and WHO was mobilized from the Global Outbreak Alert and Response Network; the team arrived in Madagascar on August 14. This report summarizes the preliminary epidemiologic and virologic findings, which suggest that the outbreak was attributable to influenza A (H3N2) viruses. Further surveillance and research about the epidemiology of influenza in Madagascar is planned. Nationwide surveillance for influenza-like illness (ILI) cases implemented by MOH suggested that the outbreak peaked during the week of August 22. As of September 19, the outbreak appeared to be over, with 30,304 cumulative cases and 754 deaths reported from 13 of 111 health districts and four of six provinces (Figure 2); approximately 85% of cases were reported from Fianarantsoa Province. The majority of illnesses occurred in rural areas, and 95% of deaths occurred away from health facilities and could not be investigated. No standardized case definition was used, and the degree of overreporting or underreporting of ILI cases is uncertain. Field investigations were conducted in three highland districts of Fianarantsoa Province in which high numbers of cases and deaths had been reported. The investigations' objectives were to confirm the etiology of the outbreak and to make recommendations based on the epidemiologic findings. An analysis of ARI data from 1999--2002 collected at health centers indicated that ARI cases in highland districts peaked each year during the winter months of May--September. The peaks in ARI cases coincided with peaks of mortality from all causes and from respiratory conditions such as pneumonia during 1999--2002. In Ikongo District (estimated 2002 population: 161,494) of Fianarantsoa Province, the numbers of ARI cases evaluated at health centers and deaths from all causes that occurred during July--August were substantially higher than those that occurred during identical periods in previous years. However, the ratio of deaths to ARI cases appeared to be similar to proportions recorded during previous years. In three communes of Ikongo District (estimated 2002 population: 58,037), 54% of the reported deaths attributed to ARI that occurred during July--August were among children aged <5 years, but the highest mortality rate was among persons aged >60 years. A survey of a remote village (population: 750) in Ikongo District indicated an ARI attack rate of 67% and an estimated case-fatality ratio of 2%. In contrast, no unusually high morbidity or mortality was reported among the population of Fianarantsoa Province's capital city or in Antananarivo (estimated 2002 population: 1.25 million), where morbidity and virologic surveillance for influenza is conducted all year by IPM. During July 19--August 22, a total of 152 respiratory specimens were collected for viral isolation from ill persons in three areas of Fianarantsoa Province (Sahafata, Ikongo, and Manandriana) where outbreaks occurred. The international team also used rapid influenza-antigen tests to test specimens in the field. Influenza A viruses were isolated from specimens collected from ill persons in each area that was investigated; 27 influenza isolates were characterized antigenically at IPM and confirmed by the WHO Collaborating Centre for Reference and Research on Influenza, London, United Kingdom; all isolates were A/Panama/2007/99-like (H3N2) viruses. The A (H3N2) component of both the 2002 Southern Hemisphere and 2002--03 Northern Hemisphere influenza vaccines are well matched to the outbreak strain. Reported by: L Rasoazanamiarina, MD, A Lamina, MD, Ministry of Health; M Andrianarivelo, MD, G Razafitrimo, Institut Pasteur; A Ndikuyeze, MD, B Andriamahefazafy, MD, World Health Organization, Antananarivo, Madagascar. C Paquet, MD, International Health Dept, I Bonmarin, MD, Infectious Diseases Dept, Institut de Veille Sanitaire, Saint-Maurice, France. J Manuguerra, PhD, Molecular Genetics Unit for Respiratory Viruses, National Reference Center for Influenza, Institut Pasteur, Paris, France. B Koumare, PhD, World Health Organization Regional Office for Africa, Brazzaville, Congo. N Shindo, MD, K Stohr, PhD, K Ait-Ikhlef, Dept of Communicable Disease Surveillance and Response, World Health Organization, Geneva, Switzerland. T Uyeki, MD, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases, CDC. Editorial Note:The epidemiologic and virologic data suggest that the large outbreak described in this report was attributable to influenza A/Panama/2007/99-like (H3N2) viruses, which have been in circulation worldwide for several years. Influenza outbreaks in remote regions have been reported rarely (1--4). Several factors might have contributed to the widespread ARI morbidity and unusually high mortality reported from rural highland regions during this outbreak. In remote villages, crowded living conditions during an unusually cold and wet winter might have facilitated person-to-person transmission of influenza among highly susceptible populations. Fianarantsoa Province is one of the poorest regions of Madagascar; malnutrition is prevalent, and access to health care is poor. These factors might have been exacerbated further by civil unrest during December 2001--June 2002. This outbreak illustrates several important lessons for controlling influenza outbreaks in developing countries and for global pandemic influenza planning. Because the outbreak occurred primarily in remote areas, awareness of the outbreak and response by health authorities were delayed. Although influenza surveillance is conducted in Antananarivo by IPM's WHO-recognized National Influenza Center, no data were available for the most affected areas. In Madagascar, as in many developing countries, efforts to assess and control the outbreak were complicated by at least seven factors: 1) malnutrition, 2) poor access to health care in remote areas, 3) difficulties in reaching rural populations, 4) limited communicable disease surveillance, 5) shortages of antibiotics to treat secondary bacterial complications, 6) the unavailability of influenza vaccine, and 7) lack of awareness about influenza. In addition, limited influenza surveillance has prevented an understanding of the epidemiology and impact of influenza in many developing countries, especially in Africa (5). In response to this outbreak, the team recommended expanding influenza surveillance, educating the public and health-care providers about influenza, improving access to health care in rural areas, and ensuring that adequate supplies of antibiotics are available at health-care centers to treat bacterial complications of influenza. Influenza vaccination was not recommended because the outbreak was already widespread in August, and the ability to distribute vaccine in remote areas was extremely limited. Members of the international team plan to return to Madagascar to assist MOH to better characterize the outbreak. Acknowledgments This report is based on contributions by R Migliani, MD, M Ratsitorahina, PhD, P Grosjean, N Rasolofonirina, MD, L Rabarijaona, MD, Institut Pasteur, Antananarivo; D Rabdrianasolo, MD, C Ravaonjanahary, PhD, M Ratolojanahary, MD, Ministry of Health; J Rasamizanaaka, MD, H Ravokatsoa, MD, L Razafilahy, Dept of Public Health, Fianarantsoa Province; B Tanjaka, MD, Ikongo District; P Rakotoarisoa, MD, Manadriana District; E Raharilalao, MD, Anjoma, Nadihizana District, Madagascar. C Bouchier, PhD, V Lorin, Institut Pasteur, Paris, France. A Hay, PhD, World Health Organization Collaborating Center for Reference and Research on Influenza, London, United Kingdom. R Arthur, PhD, M Ryan, MD, World Health Organization Global Alert and Response Team, Communicable Disease Surveillance and Response Dept, Geneva, Switzerland. S Harper, MD, K Fukuda, MD, J LeDuc, PhD, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases, CDC. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 11/14/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 11/14/2002