|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
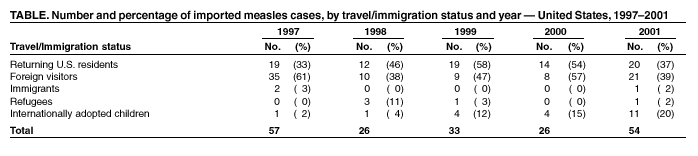
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Measles Outbreak Among Internationally Adopted Children Arriving in the United States, February--March 2001On February 16, 2001, the Texas Department of Health was notified about a child aged 10 months adopted from orphanage A in China who was taken to a Texas hospital with fever, conjunctivitis, coryza, Koplik spots, and a maculopapular rash. Measles was confirmed by serologic testing. Public health authorities in Texas notified CDC, which then collaborated with health officials in other states to contact other recently adopted children from China and their adoptive families. This report summarizes the results of multistate contact investigations that identified 14 U.S. measles cases and outlines measures taken in the United States and China to control and prevent measles transmission. The index patient had traveled with prodromal fever on international (China to Los Angeles) and domestic (Los Angeles to Houston) flights on commercial airlines and had been part of a cohort of adopted children from China who had resided in orphanage A. These children and their adoptive families had spent >2 weeks together in China while the families were visiting the orphanage and completing the immigrant visa process. The index patient potentially exposed multiple persons during the communicable period, including members of 63 families who had traveled to China to adopt children, representatives from 16 international adoption agencies who accompanied the families, staff at the local medical facility in China at which the patient was examined as a requirement for a U.S. immigrant visa, staff at the U.S. Consulate, passengers and crew members of the international and domestic flights on which the patient traveled, and adoption-agency representatives who met the returning family. By February 22, consulate staff in China, staff at the medical facility, administrators at orphanage A, and all adoption agencies involved received information from CDC about measles exposure and prevention. Through the U.S. Consulate in China, the Central China Adoption Agency (CCAA) and CDC developed a collaborative strategy to control and prevent further spread of measles. The strategy included nine steps: 1) retrospective notification of families of adopted children from orphanage A who were interviewed at the U.S. Consulate during January 30--February 12; 2) prospective notification of families planning to travel to orphanage A advising them to delay travel to China until further notice; 3) distribution of alerts to adoptive families already in China; 4) notification of international adoption agencies in China to advise prospective adoptive families to verify and update the vaccination status of household members; 5) active screening for febrile and rash illnesses among adopted children examined at the medical facility in China; 6) isolation of children suspected to have measles and restriction of their travel on commercial conveyances; 7) temporary suspension of adoption proceedings at orphanage A until no new measles cases were identified; 8) evaluation of children at orphanage A for measles; and 9) initiation of a vaccination campaign in orphanage A under the direction of CCAA. Contact investigations identified 14 U.S. measles cases (13 confirmed serologically and one linked epidemiologically) among children who were recently adopted from China and their family members and close contacts in eight states, including 10 recently adopted children aged 9--12 months from seven states (New York [three], Ohio [two], Illinois [one], Indiana [one], Minnesota [one], Missouri [one], and Texas [one]), two U.S.-born adoptive mothers (Indiana [aged 46 years] and Missouri [aged 39 years]), a U.S.-born caretaker (Connecticut [aged 47 years]) who had lived for a week in the same household as an adopted child with measles, and a sibling (Georgia [aged 28 months]) of a healthy adopted child from China. Thirteen U.S. measles cases were imported; the case of the U.S.-born caretaker was an indigenous, import-linked case. All 14 cases of measles were identified during multistate investigations during February--March 2001. Among the 13 imported cases in adopted children and their family members, dates of onset of measles rash ranged from February 15 to March 7, 2001. These dates suggest incubation periods consistent with measles exposure in China, most likely at orphanage A but possibly during the medical screening or travel. The one indigenous, epidemiologically linked measles case was consistent with secondary transmission of measles in the United States from an adopted child. During the investigation, representatives of orphanage A retrospectively identified cases of suspected measles that preceded the index patient's illness and reported that newly arrived children at orphanage A had not been vaccinated adequately against measles. After completion of a measles vaccine campaign at orphanage A, no additional cases were reported, and the adoption of children from the orphanage resumed on March 29, a total of 3 weeks after the onset of the last known case of measles. Reported by: A Reynolds, T Gong, U.S. Consulate; H Li, MD, International Travelers Health Care Center, Guangzhou, China. K Hendricks, MD, J Pelosi, MPH, Texas Dept of Health. S Lance-Parker, DVM, Georgia Div of Public Health. W Staggs, MS, Indiana State Dept of Health. C Miller, MS, Minnesota Dept of Health. G Storm, V Tomlinson, MPH, Missouri Dept of Health. E Herlihy, MS, New York State Dept of Health. C Jennings, K Hunt, Illinois Dept of Public Health. F Smith, MD, J Daniels, MD, Ohio Dept of Health. Div of Global Migration and Quarantine, National Center for Infectious Diseases; Div of Epidemiology and Surveillance, National Immunization Program, CDC. Editorial Note:During 1997--2001, the annual number of reported measles cases in the United States ranged from 86 to 138, with imported cases accounting for 26%--47% of the total (Table). The proportion of imported cases of measles among internationally adopted children increased from 2% in 1997 to 20% in 2001; 10 of the 11 imported cases of measles among internationally adopted children in 2001 were associated with this outbreak. During fiscal year 2001, the U.S. Immigration and Naturalization Service reported that 19,230 internationally adopted children, of whom 4,681 (24%) were from China, were admitted to the United States. Imported cases of measles continue to infect susceptible U.S. residents. The current high level of immunity to measles in U.S. residents and the coordinated efforts of numerous agencies in responding to imported cases has limited indigenous spread. Three (23%) of 13 imported measles cases in this investigation were in U.S. residents returning from abroad and constituted 6% of all imported cases for 2001, underscoring the need for U.S. residents to verify their immunity against measles before international travel. The criteria for immunity to measles are 1) having been born before 1957, 2) a history of physician-diagnosed measles, 3) documentation of having received 2 doses of measles-containing vaccine, or 3) serologic evidence of measles immunity. Travelers who are not immune should be vaccinated (1). Since 1996, all persons seeking a U.S. immigrant visa are required to show proof of having received at least the first vaccine of each series of vaccinations recommended by the Advisory Committee on Immunization Practices (ACIP), which includes measles (2). However, internationally adopted children who are aged <10 years are exempted from the Immigration and Nationality Act vaccination requirements with a signed statement from the adopting parent(s) indicating that the child will receive vaccination within 30 days of entry into the United States. Parents of internationally adopted children should be aware of the importance of confirming that they and their family members are current in their vaccinations and that, soon after arrival in the United States, their adopted children's vaccination status is updated according to ACIP guidelines (1). In addition, persons who will be in contact with internationally adopted children during their first 3 weeks in the United States, especially household members and caretakers, should be immune to measles or be vaccinated before the adoption. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
Page converted: 12/12/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 12/12/2002