|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
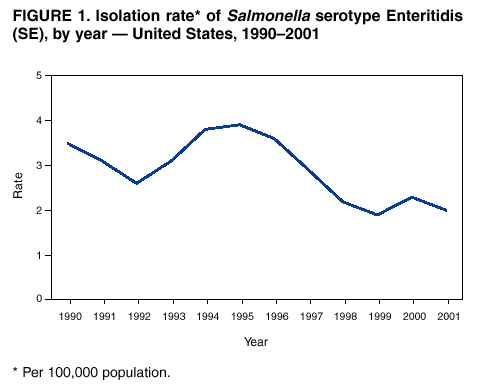
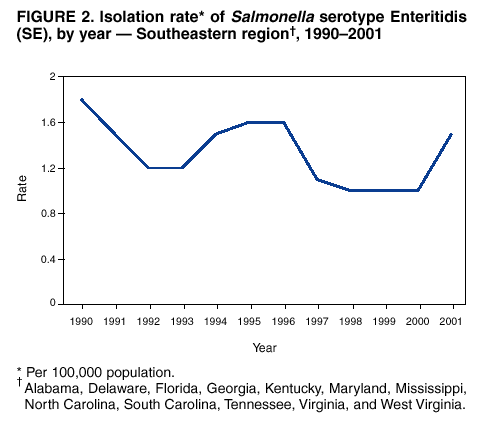
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreaks of Salmonella Serotype Enteritidis Infection Associated with Eating Shell Eggs --- United States, 1999--2001A Salmonella serotype Enteritidis (SE) epidemic emerged in the 1980s, when increasing numbers of infections were detected in the Northeastern and Mid-Atlantic regions of the United States (1). In the early 1990s, while SE rates in the Northeast began to decline, the SE epidemic expanded to the Pacific region (2). Nationwide, the number of SE isolates reported to CDC peaked at 3.8 per 100,000 population in 1995. Although rates of culture-confirmed SE infection reported to CDC declined to 1.9 by 1999 (Figure 1), rates did not decline further through 2001, and outbreaks continue to occur. Investigations of outbreaks and sporadic cases have indicated repeatedly that, when a food vehicle is identified, the most common sources of SE infection are undercooked and raw shell eggs (3,4). This report describes two SE outbreaks associated with eating shell eggs and underscores the need to strengthen SE-control measures. South Carolina, 2001During February--March 2001, outbreaks of gastroenteritis occurred among inmates in four prison facilities of the South Carolina Department of Corrections (SCDC). The first outbreak occurred in a men's facility (M1) on February 6. The three other outbreaks, all occurring on March 2, affected a second men's facility (M2) and two women's facilities (F1 and F2). Among 2,317 inmates in the four prisons, 688 reported to prison infirmaries with gastrointestinal symptoms (e.g., abdominal cramps, diarrhea, and nausea). Stool specimens from ill inmates yielded SE phage types 2, 13a, and 23. No illness was reported among SCDC staff members. The South Carolina Department of Health and Environmental Control conducted two case-control studies in M2 and F1, which shared a common kitchen. A case-patient was defined as any SCDC inmate who reported to the prison infirmary with acute gastrointestinal symptoms. Case-patients were selected at random from a list of ill inmates. Controls were inmates without illness who were selected at random from an inmate roster provided by the prisons and who were matched by prison facility. A tuna salad served for lunch on March 2 was eaten by 88% of the male case-patients (odds ratio [OR]=7.0; 95% confidence interval [CI]=1.8--30.5) and by 89% of the female case-patients (OR=16.7; 95% CI=4.1--74.7). The tuna salad was prepared with eggs that were reportedly hard-boiled by kitchen staff, who also were inmates. At the time of the outbreaks, all eggs used by the four involved SCDC facilities were supplied from a single vendor. Eggs supplied to M2 and F1 were traced back to the vendor's farm (Farm A). In February 2001, eggs submitted from Farm A to the South Carolina Egg Quality Assurance Program tested positive for SE phage types 2,13a, 22, 23, and 28. Phage type 2 was the predominant SE strain isolated from both ill patients and eggs from Farm A. To protect the inmates, SCDC switched to pasteurized egg products in April 2001. North Carolina, 2001In June 2001, the Statistical Outbreak Detection Algorithm at CDC signaled an increase in SE cases reported from North Carolina. The Division of Public Health in North Carolina was alerted and began to review SE cases throughout the state. The North Carolina State Laboratory of Public Health reported 51 cases in July and 31 in August, compared with 11 cases in each of those months during 2000. Cases occurred throughout the state. A case-control study was performed. A case was defined as culture-confirmed SE in a resident of North Carolina reported during July 1--September 7, 2001. One to two neighbor controls were matched to each case. SE isolates were subtyped by pulsed-field gel electrophoresis (PFGE) and phage typing. Analysis of 53 patients and 78 controls indicated that illness was associated with eating eggs (matched odds ratio [MOR]=2.8; 95% CI=1.1--9.5). Isolates from 21 (40%) of 53 patients had PFGE pattern A. Analysis restricted to patients with pattern A indicated a stronger association with egg consumption (MOR=10.7; 95% CI=1.3--88.1). PFGE pattern A also was identified in isolates from patients in the South Carolina SE outbreak. All isolates from SE patients in both outbreaks that were PFGE pattern A also were phage type 13a. Among 14 random, nonoutbreak phage type 13a SE isolates tested subsequently at CDC, seven distinct PFGE patterns were identified; none was PFGE pattern A. A traceback of implicated eggs purchased from retail outlets in North Carolina was inconclusive for implicating a farm. Reported by: D Drociuk, MSPH, S Carnesale, MD, G Elliot, LJ Bell, MD, JJ Gibson, MD, South Carolina Dept of Health and Environmental Control. L Wolf, D Briggs, B Jenkins, JM Maillard, MD, North Carolina Dept of Health and Human Svcs. M Huddle, MPH, F Virgin, C Braden, MD, Div of Bacterial and Mycotic Diseases, National Center for Infectious Diseases; P Srikantiah, MD, A Stoica, MD, T Chiller, MD, EIS officers, CDC. Editorial Note:During 1990--2001, state and territorial health departments reported 677 SE outbreaks, which accounted for 23,366 illnesses, 1,988 hospitalizations, and 33 deaths (CDC, unpublished data, 2002). Among the 309 outbreaks reported with a confirmed vehicle of transmission, 241 (78.0%) were associated with shell eggs, accounting for 14,319 illnesses. Of these, 10,406 illnesses occurred during 1990--1995, and 3,913 occurred during 1996--2001. The overall decrease in SE incidence and the decrease in the number of illnesses related to egg-associated SE outbreaks during the last decade might be attributed in part to the implementation of prevention measures, including on-farm control programs, egg refrigeration, and consumer and food worker education. However, reported cases did not decline during 1999--2001, and outbreaks associated with shell eggs continue to occur. In the South Carolina outbreak, eggs from a farm that tested positive for SE in February 2001 were distributed to the prisons in March, despite the farm's participation in a voluntary, state-sponsored SE-control program. This farm withdrew from the state program in April 2001. Phage type 2 was the most common SE strain isolated in the South Carolina outbreak. This uncommon phage type, which has accounted for 3% of SE outbreaks with reported phage type since 1985, also was found on Farm A. Cases in the outbreak in North Carolina shared the same SE PFGE pattern and phage type (13a) as some of the South Carolina outbreak cases, suggesting a possible link to the same farm. Eggs that reportedly were hard-boiled and used in a tuna salad were the implicated vehicle in the South Carolina outbreak. A recent study demonstrated that unless SE-containing eggs are exposed to boiling water until the yolk is completely solidified, SE can survive the cooking process (5). Cross contamination of the tuna salad by inmate food handlers also was possible. To achieve sustained decreases in egg-associated SE illnesses, a concerted prevention effort is needed from farmers to consumers (6). A key factor in this effort is the implementation of farm-based measures to reduce SE contamination of eggs during production. The implementation of such control programs in Northeastern states in the early 1990s might have contributed to subsequent decreases in human SE isolation rates in New England and Mid-Atlantic regions (7). One important control measure is microbiologic testing of hen houses for the presence of SE. If SE is found on a farm during routine environmental testing, eggs may be diverted to pasteurization. Evidence suggests that proper implementation and oversight of farm-based control programs can result in a reduction of SE infections among flocks in poultry houses (8). Farm participation in current SE-control programs is voluntary, and the components of programs vary. Future shell-egg safety measures should include greater participation in farm-based control programs with microbiologic testing. Both outbreaks described in this report occurred in the Southeastern region of the United States. Compared with declining rates of SE infections in other regions of the United States, the incidence of SE in Southeastern states increased by 50% from 2000 to 2001 (Figure 2). Ongoing surveillance of SE outbreaks will be necessary to detect changes in trends of SE infection in this region. Expansion of SE-prevention measures will be an important part of efforts to prevent SE infections in the Southeast. This includes actively encouraging farms to participate in SE-control programs, promotion of proper refrigeration of eggs during storage and transportation, and education of food handlers and consumers about food preparation (see box). Retail and consumer buyers can specify that suppliers provide only eggs produced from farms managed under an SE-control program that is recognized by a state regulatory agency or a state poultry association. The outbreak in South Carolina prisons was the largest SE outbreak in 2001. Because persons residing in institutions depend entirely on their institutions for meals, the supply of contaminated foods to these settings can place large populations at risk for developing foodborne diseases. Persons residing in institutions, especially elderly persons in nursing homes or assisted living facilities, are at higher risk for dying from outbreak-associated SE infections (9). During 1990--2001, a total of 83 SE outbreaks occurred in institutional settings*, representing 12% of reported SE outbreaks. Of the 33 outbreak-associated deaths, 22 (67%) occurred in institutional facilities, underscoring the importance of using pasteurized egg products or in-shell pasteurized eggs for all recipes requiring pooled, raw, or undercooked shell eggs for institutionalized persons. Additional information about preventing SE infections associated with eating raw or undercooked shell eggs is available at http://www.cdc.gov/ncidod/dbmd/diseaseinfo/salment_g.htm, http://www.cfsan.fda.gov/~dms/fs-eggs.html, http://www.cfsan.fda.gov/~dms/fs-eggs2.html, and http://www.cfsan.fda.gov/~dms/fs-eggs4.html. Information for retail and food service establishments and institutional facilities about handling and cooking shell eggs is available in the Food Code at http://www.cfsan.fda.gov/~dms/foodcode.html. References
* Institutional settings include nursing homes, independent living facilities, assisted living facilities, childcare settings, campus cafeterias, prisons and correctional facilities, and shelters.
Box
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 1/2/2003 |
|||||||||
This page last reviewed 1/2/2003
|