 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Use of Respiratory Protection Among Responders at the World Trade Center Site --- New York City, September 2001The terrorist attacks on the World Trade Center (WTC) on September 11, 2001, created an occupational health and safety challenge for New York City (NYC) firefighters and rescue workers responding to the disaster. Immediate respiratory hazards included explosions, fire, falling debris, and dust clouds containing particulate matter comprised of pulverized building materials. Ongoing risks included lingering particulate matter in the air and intermittent combustion products from initial and persistent fires beneath the rubble pile. Because the nature and extent of exposures in disaster situations are complex and difficult to characterize, the use of adequate personal protective equipment (PPE), including respiratory protection, is essential in protecting the health of firefighters and other rescue workers. During the weeks after September 11, the NYC Fire Department's Bureau of Health Services (FDNY-BHS) and CDC's National Institute for Occupational Safety and Health (NIOSH) organized a collaborative study to evaluate occupational hazards and exposures for these workers, including their use of respiratory protection. This report summarizes the results of that study, which indicate that the majority of firefighters did not use adequate respiratory protection during the first week of the rescue/recovery operation. The study population consisted of the approximately 11,000 FDNY firefighters present at the WTC site during the first week of the disaster. The cross-sectional study used a stratified random sample of firefighters, categorized by arrival time at the WTC. The study was conducted during October 2--5 and included a questionnaire (self-administered through touch-screen computer), medical evaluation, spirometry, and blood/urine collection for biomonitoring assays. The 53 questions elicited arrival time, number of days worked at the WTC, work activities, and use of PPE (including respiratory protection) during each day worked at the WTC during the first 2 weeks. The medical evaluation was mandatory, but participation in the research study was voluntary and required informed consent. The respiratory protection section of the questionnaire elicited firefighter respirator use during each of the five time periods: during the collapse, day 1, day 2, days 3--7, and week 2 following the collapse. The number of participants present each day was calculated and used to generate rates of respirator use for each time period by respirator type. Questionnaire choices included the following four types of respirators used by firefighters, regardless of availability: 1) self-contained breathing apparatuses (used for firefighting), 2) N95 filtering face masks (used for medical response), 3) half-face respirators,* and 4) disposable dust/paint masks (hardware store type). The disposable dust/paint mask might not have been a NIOSH-certified respirator. Of 400 firefighters, 361 (91%) participated in the study; 319 had responded to the WTC disaster, and 42 were unexposed controls. All participants were men; mean years worked as a firefighter was 15 years (range: <1--38 years), and mean age was 42 years (range: 24--60 years). The firefighters who responded to the disaster were asked whether they were present at the site during various time periods: 149 reported being present during the collapse, 118 arrived later that day, 222 were present on day 2, a total of 284 were present >1 day during days 3--7, and 231 were present during week 2. Of those present during the WTC collapse, 67 (52%) reported wearing no respiratory protection, and 41 (38%) of those arriving later that day wore no respirator (Figure). The respirator most commonly used during the first day was the disposable mask; of the 130 firefighters present on the first day (either during or following the collapse) who reported wearing a respirator, 76 (58%) used the disposable mask. During the initial 2-week period, use of half-face respirators increased, and use of the disposable masks decreased. Reported by: D Prezant, MD, K Kelly, MD, New York City Fire Dept, Bur of Health Svcs. B Jackson, PhD, D Peterson, PhD, RAND Science and Technology Policy Institute, Santa Monica, California. D Feldman, MD, S Baron, MD, CA Mueller, MS, B Bernard, MD, B Lushniak, MD, Div of Surveillance, Hazard Evaluations and Field Studies; L Smith, MS, R BerryAnn, B Hoffman, MBA, National Personal Protective Technology Laboratory, National Institute for Occupational Safety and Health, CDC. Editorial Note:Adequate planning, preparation, and training are key to protecting the safety and health of emergency responders. Anticipating the nature and magnitude of exposures during the initial stages of a disaster situation is difficult; however, plans should be in place to provide a rapid emergency response and protect the health of the responders. The findings in this report indicate that many firefighters responding to the WTC disaster were not protected adequately during the initial stages of the emergency response. The findings in this report are subject to at least two limitations. First, the collection of reliable information about respirator use patterns is difficult. Some firefighters reporting use of a respirator might not have been fit-tested adequately or might have used it sporadically, resulting in an overestimation of the percentage of those who were protected adequately. Second, because firefighters were asked to report daily respirator use 3--4 weeks after the event, responses are subject to recall bias. Despite these limitations, the general results from the questionnaire are consistent with reports by safety experts who were present during the first few weeks of the rescue/recovery operations. To evaluate the availability and adequacy of PPE during disaster situations and to make recommendations for future planning, CDC, in collaboration with the RAND Science and Technology Policy Institute, sponsored a conference of persons with first-hand knowledge of emergency response to terrorist attacks. The conference was held in NYC in December 2001. Attendees included persons who responded to the 1995 attack on the Alfred P. Murrah Federal Building in Oklahoma City, the September 11 attacks on the WTC and the Pentagon, and the anthrax incidents that occurred during fall 2001, and represented multiple occupations and skills (e.g., firefighters, police, emergency medical technicians, construction workers, union officials, and government representatives from local, state, and federal agencies). The participants discussed all aspects of a program for protection of emergency responders including information and training, performance of particular PPE in a disaster environment, and concerns related to adequate management of disaster sites. On the basis of this experience, participants developed recommendations about technologies and procedures that could help protect the health and safety of emergency workers as they respond to acts of terrorism. The final recommendations included the following (1): PPE Performance
PPE Availability
Training and Information
Management
Acknowledgment This report was based on data contributed by S Lenhart, MSPH, Div of Surveillance, Hazard Evaluations and Field Studies, National Institute for Occupational Safety and Health, CDC. Reference1. RAND Science and Policy Institute. Protecting emergency responders: lessons learned from terrorist attacks. Santa Monica, California: RAND Science and Policy Institute, 2002. Available at http://www.rand.org/publications/CF/CF176. *The half-face elastomeric reusable respirator with combination P100 and organic vapor/acid gas cartridges were recommended by NIOSH and other agencies for WTC rescue/recovery personnel working in debris or performing decontamination at the WTC site (work in which surface dust was disturbed or resuspended in the air). For workers not scheduled to work in debris, a half-face P100 or N100 respirator (either disposable or elastomeric) was recommended; however, these were not available routinely during the initial 48 hours.
Figure 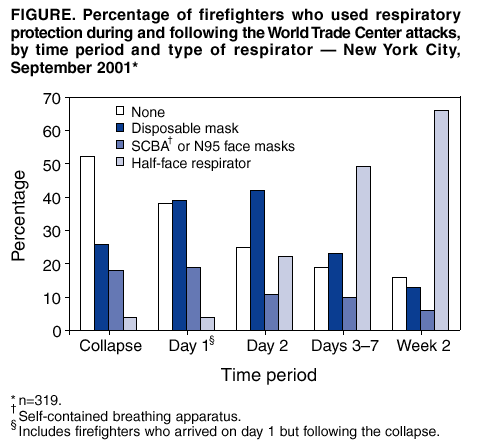 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 9/9/2002 |
|||||||||
This page last reviewed 9/9/2002
|