|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
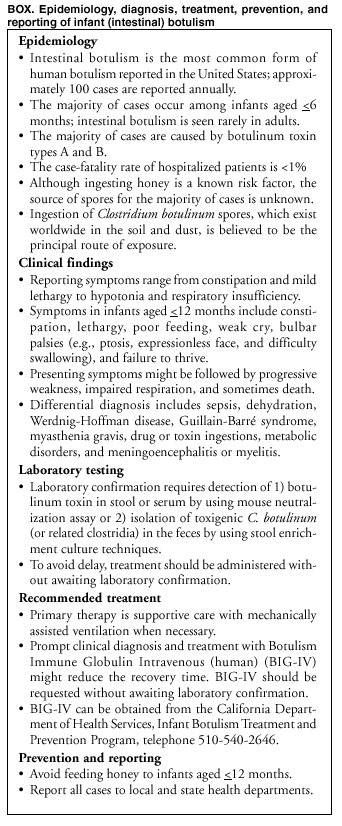
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Infant Botulism --- New York City, 2001--2002Infant botulism results from germination of swallowed spores of botulinum toxin--producing clostridia that colonize the large intestine temporarily. Four cases of type B infant botulism in one New York City (NYC) borough were diagnosed within a 12-month period during 2001--2002. All four patients resided in Staten Island (2000 population: 443,728). The annual incidence of infant botulism in the United States is two cases per 100,000 live births; incidence in NYC is four cases per 100,000 live births. Staten Island recorded 5,899 live births in 2000; incidence of infant botulism during this 12-month period was 68 cases per 100,000 live births. This report summarizes the investigation of these four cases; as expected with infant botulism, a common source of exposure was not identified. All four patients recovered after treatment and were discharged from local hospitals. State and local health departments should be notified promptly when infant botulism is suspected to arrange diagnostic testing. Infant botulism is a reportable disease in NYC, and the NYC Department of Health and Mental Hygiene (DOHMH) investigates all suspected cases. Botulism should be suspected in an infant aged <12 months with symptoms including constipation, lethargy, poor feeding, weak cry, bulbar palsies, and failure to thrive. These symptoms might be followed by progressive weakness, impaired respiration, and sometimes death. Laboratory diagnosis of clinically suspect cases requires detection of botulinum toxin in stool or serum by using the mouse neutralization assay or the isolation of toxigenic Clostridium botulinum (or related toxigenic clostridia) in the feces by using enrichment culture techniques (1). When botulism is suspected, clinical specimens are forwarded to the DOHMH Public Health Laboratory for toxin detection. Parents or caregivers are interviewed by using a standardized questionnaire on clinical symptoms and risk factors, and the physician is interviewed or charts are abstracted for information on signs and symptoms. Case ReportsCase 1. In June 2001, a previously healthy breast-fed infant aged 7 weeks with fever of 105º F (41º C), constipation, listlessness, poor feeding, and weak head control for 1 day was admitted to a New Jersey hospital. The infant was irritable and had sluggishly reactive pupils, altered cry, somnolence, respiratory weakness, and upper airway obstruction that necessitated mechanical ventilation for 13 days. Botulinum toxin type B was identified 8 days after illness onset in stool samples at the New Jersey Public Health and Environmental Laboratories. The family had spent time at residences in Staten Island and New Jersey before illness onset. The patient was discharged after 26 days without sequelae and recovered fully. Case 2. In December 2001, a formula-fed infant aged 10 weeks with a history of constipation in the first month of life was admitted to a hospital after having difficulty in sucking and swallowing for 2 days. Mechanical ventilation was required for 10 days because of respiratory failure. The infant was irritable and had loss of facial expression, generalized muscle weakness, and constipation. A diagnosis of infant botulism was established 29 days after onset of symptoms by detection of toxin type B in stool enrichment cultures. The patient was treated with Botulism Immune Globulin Intravenous (human) (BIG-IV) and discharged after 20 days; the infant recovered fully. Case 3. In May 2002, a previously healthy breast-fed infant aged 18 weeks had somnolence and difficulty swallowing for 1 day. The infant was admitted to a hospital and subsequently had altered cry, loss of facial expression, respiratory muscle weakness, and upper airway obstruction that necessitated mechanical ventilation for 8 days. The patient also had an intussusception without a recognizable lead point (2). A diagnosis of botulism was established 19 days after onset of symptoms by detection of toxin type B in stool enrichment cultures. The patient was treated with BIG-IV and discharged after 16 days; the infant recovered fully. Case 4. In June 2002, a previously healthy infant aged 3 weeks who was both breast- and formula-fed had constipation, lethargy, and decreased appetite for 2 days; the infant was brought to a hospital for evaluation and was admitted the following day. The infant was irritable and had sluggish pupillary reflexes, difficulty swallowing, altered cry, weak sucking, and peripheral weakness. A diagnosis of botulism was established 8 days after onset of symptoms by detection of toxin type B in stool samples. The patient was treated with BIG-IV and discharged after 10 days; the infant recovered fully. Summary of CasesAll four patients received antibiotics during hospitalization. None had ingested honey or had parents employed in occupations that might increase exposure to C. botulinum spores in soil and dust (e.g., construction, plumbing, and farming) (3). All patients had uncomplicated gestational histories and vaginal deliveries. All resided within a 6-mile radius of each other. All parents reported recent construction in their neighborhoods during the period (range: 1--31 days) before illness onset. In the fourth case, the infant's home had been remodeled since the infant was born. On May 30, 2002, after three cases had been identified by routine passive surveillance, DOHMH alerted local physicians by broadcast facsimile and e-mail about the increased rate of infant botulism in Staten Island. Physicians were reminded to consider the diagnosis and to report suspected cases to DOHMH to request assistance with diagnostic testing. Physicians were directed to contact the California Department of Health Services (CDHS) Infant Botulism Treatment and Prevention Program about possible treatment with BIG-IV under a Food and Drug Administration (FDA)--approved protocol (4). All parents of patients in Staten Island were reinterviewed by using an expanded questionnaire and visited in their homes and neighborhoods to assess for possible common sources of exposure; no such source was identified. Reported by: V Reddy, MPH, S Balter, MD, D Weiss, MD, M Layton, MD, Bur of Communicable Diseases; L Kornstein, PhD, Public Health Laboratory, New York City Dept of Health and Mental Hygiene, New York, New York. I Friberg, MHS, R Schechter, MD, S Arnon, MD, Infant Botulism Treatment and Prevention Program, California Dept of Health Svcs. MJ Hung, MSW, E Bresnitz, MD, New Jersey Dept of Health and Senior Svcs; K Pilot, S Matiuck, New Jersey Public Health and Environmental Laboratories. J Sobel, MD, Div of Bacterial and Mycotic Diseases, National Center for Infectious Diseases; M Phillips, MD, EIS Officer, CDC. Editorial Note:Intestinal botulism is the most common form of human botulism in the United States (1), and approximately 100 cases are reported among infants in the United States annually (Box. Intestinal botulism occurs rarely in older children and adults (2,5,6). Intestinal botulism results from colonization and bacterial production of botulinum toxin in the colon. Swallowing ambient C. botulinum spores, which exist worldwide in soil and dust, has been proposed as the principal route of exposure; honey is an avoidable source of some causative spores (4). A common source of exposure generally is not identified; apparent clusters such as the four Staten Island cases are rare and often remain unexplained after investigations are complete (7). In a cluster of infant botulism cases identified previously in the mid-Atlantic region of the United States, no common source of exposure was identified (8). Botulism should be suspected in previously healthy infants aged <12 months who are constipated and who exhibit weakness in sucking, swallowing, or crying; hypotonia; and progressive bulbar and extremity muscle weakness. Approximately half of patients require mechanical ventilation during hospitalization (9). Lumbar puncture and brain imaging generally yield normal results but can help differentiate among other causes of flaccid weakness. When infant botulism is suspected, local and state health departments should be notified promptly to arrange diagnostic stool testing. The primary therapy for infant botulism is intensive care with mechanically assisted ventilation when necessary. Prompt diagnosis and treatment of infant botulism with BIG-IV might reduce the length of time needed for recovery. In a placebo-controlled trial of BIG-IV, the mean hospital stay of patients with infant botulism was reduced from 5.6 to 2.6 weeks (4). Therapy is guided by clinical diagnosis; to avoid delay in treatment, BIG-IV should be requested and administered without awaiting laboratory confirmation. BIG-IV can be obtained from the CDHS Infant Botulism Treatment and Prevention Program, telephone 510-540-2646. Use of BIG-IV under the FDA-approved Treatment Investigational New Drug open-label protocol requires informed parental consent and coordination with the hospital's institutional review board (IRB). The license application for BIG-IV was filed with FDA in 2001; should it be licensed, IRB approval would no longer be required. Infant botulism is notifiable at the national level, and physicians should report all cases promptly to state and local health departments. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 1/16/2003
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 1/16/2003