|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
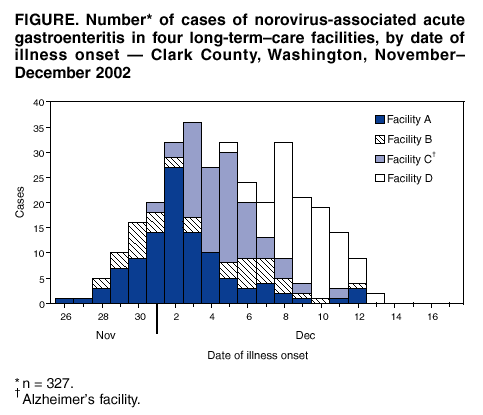
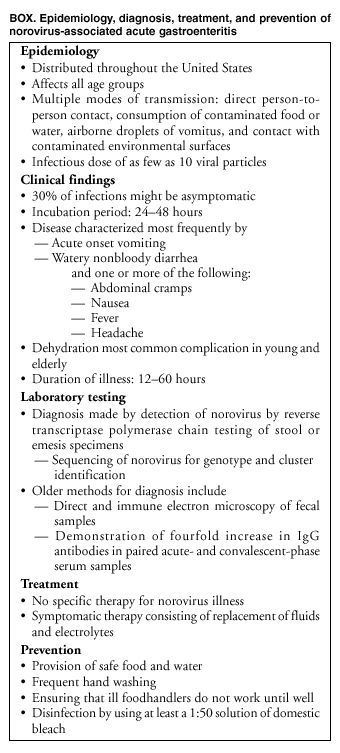
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Norovirus Activity --- United States, 2002Please note: An erratum has been published for this article. To view the erratum, please click here. During June--December 2002, an increased number of outbreaks of acute gastroenteritis (AGE) were reported on cruise ships sailing into U.S. ports (1). In addition, since October 2002, several states have noted an increase in outbreaks of AGE consistent clinically and epidemiologically with norovirus infection, particularly in institutional settings such as nursing homes (CDC, unpublished data, 2002). This report describes recent norovirus activity in two states and New York City (NYC) and data from CDC that indicate the possible emergence of a predominant, circulating norovirus strain. WashingtonDuring November--December 2002, the Southwest Washington Health District, Clark County, Washington, received reports of 10 outbreaks of AGE affecting 354 patients from six long-term--care facilities (LTCFs), a community hospital, an outpatient clinic, and the county jail. Outbreaks in four LTCFs accounted for 327 (92%) of the cases, including 220 (49%) among 452 residents and 107 (33%) among 326 staff. Onset of illness for all patients occurred during November 26--December 13 (Figure). For all 354 patients, illness was characterized by diarrhea (84%), nausea (78%), and vomiting (77%). The mean duration of illness was 49 hours (range: 20--72 hours); mean duration of outbreak in the four LTCFs was 12 days (range: 9--16 days). Eight ill persons were hospitalized. Three of the four LTCFs included residents receiving various levels of care (i.e., nursing care). The fourth LTCF provided care exclusively for persons with Alzheimer's disease and experienced the highest attack rates (ARs) for residents (AR: 85%) and staff (AR: 41%), compared with the other three LTCFs (AR among residents: 42%; AR among staff: 30%). The range of dates of illness onset in each outbreak suggests person-to-person transmission. The incubation period was 24--48 hours. Six of seven stool specimens from ill patients in these four outbreaks were positive for norovirus by reverse transcriptase-polymerase chain reaction (RT-PCR) tests performed at Washington State Public Health Laboratories and included at least one positive specimen from each of the four outbreaks. Public health nurses visited all affected LTCFs to help implement control measures, including confining ill residents to their rooms and excluding ill staff from work until 48 hours after recovery; emphasizing hand hygiene for staff in accordance with recent CDC recommendations (2); disinfecting environmental surfaces with 10% bleach solution; and postponing visits from elderly persons, very young children, and persons with underlying medical conditions. The number of cases declined in all four LTCFs after these interventions. New HampshireDuring 2002, the New Hampshire Department of Health and Human Services (NHDHHS) investigated 35 outbreaks of AGE consistent clinically and epidemiologically with norovirus infection from LTCFs and assisted-living facilities (n=29), restaurants (n=two), schools (n=two), and residential summer camps (n=two). Of the 29 outbreaks in LTCFs and assisted-living facilities, 28 were reported during November--December 2002. In 10 (29%) outbreaks, an etiology of norovirus was confirmed by RT-PCR testing of fecal specimens at NHDHHS or CDC, and 25 (71%) outbreaks were attributed to norovirus based on epidemiologic criteria (3). A total of 2,312 persons had AGE during the 35 norovirus outbreaks, resulting in 13 hospitalizations; two ill patients in LTCFs died. Epidemiologic investigation implicated person-to-person, foodborne, and waterborne transmission in 32, two, and one outbreak, respectively. Control measures in the LTCFs and assisted-living facilities included frequent and thorough hand washing, rapid cleaning of soiled areas, excluding ill staff from work for 48 hours after resolution of symptoms, ceasing of group activities, and stopping new admissions into the facilities. New Hampshire's Emergency Department Syndromic Surveillance System also detected an increase in emergency department (ED) visits for gastrointestinal illness during December 2002. In response, NHDHHS alerted all state hospitals, which increased testing for norovirus by the state laboratory. Since January 1, 2003, an additional 11 norovirus outbreaks have been reported in institutional settings; investigations are ongoing. New York CityDuring November 6, 2002--January 13, 2003, a total of 66 outbreaks of AGE consistent epidemiologically with norovirus infection occurred in NYC and were reported to the NYC Department of Health and Mental Hygiene (DOHMH) or the New York State Department of Health (NYSDOH). The outbreak settings included 51 nursing homes, LTCFs, and rehabilitation facilities; 10 hospitals; three restaurants; one homeless shelter; and one school. Approximately 1,700 persons were affected. Twenty-nine stool specimens were collected from ill patients during outbreaks in the facilities and were tested for norovirus by RT-PCR performed either at YSDOH Wadsworth Center or CDC. Nineteen (66%) specimens tested positive for norovirus, one to 10 positive specimens from each of the six outbreak settings. Control measures implemented throughout all 51 residential facilities included appropriate hand washing techniques, rapid cleaning of contaminated areas, and exclusion of ill persons from institutional and congregate settings (e.g., schools and child care centers) until 48 hours after symptoms resolved. On November 8, 2002, through its Emergency Department Syndromic Surveillance System, DOHMH detected a sustained citywide increase in ED visits from patients with diarrhea and vomiting. Through broadcast facsimile and e-mail, DOHMH alerted physicians to collect and send specimens for diagnostic testing for norovirus in all patients with AGE illness. Physicians also were encouraged to counsel patients about appropriate control measures. To identify an etiologic agent, DOHMH field staff were sent to EDs at two hospitals in areas with higher numbers of patients with AGE. Three of four stool specimens collected from patients reporting to EDs were positive for norovirus. CDC Laboratory SurveillanceDuring May--December 2002, CDC received stool specimens from 48 outbreaks of AGE in the United States. Outbreak settings included restaurants and catered events (n=12), cruise ships (n=nine), schools and child care centers (n=seven), LTCFs and assisted-living facilities (n=five), residential camps (n=two), sporting events (n=two), and other (n=11). Specimens from 37 outbreaks were tested for norovirus by RT-PCR; specimens from 11 outbreaks were unsuitable for testing by RT-PCR. Initial RT-PCR testing by using degenerate primers targeted to a 213-base region of the polymerase gene (Region B) (4--6) identified norovirus in specimens from 27 (73%) of the 37 outbreaks. Genetic characterization, based on sequencing of a different 277-base pair region of the capsid gene (Region C) (5,6), found that 11 (41%) of the 27 norovirus-positive outbreaks were associated with the same strain of norovirus. This lineage within genogroup II, cluster 4 (GII/4) (4,5) has been provisionally named the Farmington Hills strain, after Farmington Hills, Michigan, where the first cases with this norovirus strain were identified. Six of the 11 outbreaks associated with the Farmington Hills strain of norovirus occurred on land in five states (Arkansas, Georgia, Kentucky, North Carolina, and Utah). The remaining five outbreaks were associated with cruise ships. No epidemiologic link has been identified between land and cruise ship outbreaks. In addition, specimens from two of the six norovirus-positive outbreaks in NYC and the three norovirus-positive specimens collected in NYC EDs were sequenced further at CDC. The Farmington Hills strain was identified in one of the two outbreaks and two of the three single specimens. Reported by: L Anderson, MD, S Miller, MPH, J Greenblatt, MD, New Hampshire Dept of Health and Human Svcs. L Steiner-Sichel, MPH, V Reddy, MPH, R Heffernan, MPH, D Cimini, MPH, S Balter, MD, D Weiss, MD, M Layton, MD, Bur of Communicable Disease; A Agasan, PhD, M Backer, A Ebrahimzadeh, PhD, Public Health Laboratory, New York City Dept of Health and Mental Hygiene; M Kacica, MD, C Scott, Bur of Communicable Disease Control; N Chatterjee, PhD, P Smith, MD, M Fuschino, Wadsworth Center, New York State Dept of Health. M Bhat-Gregerson, E Forsyth, KR Steingart, MD, P Pace, M Payne, M Johnson, Clark County Health Dept, Washington. J Massey, PhD, Michigan Dept of Community Health. MA Widdowson, VetMB, JS Bresee, MD, RI Glass, MD, U Parashar, MD, S Monroe, PhD, RS Beard, H White, MS, L Hadley, PhD, S Bulens, MPH, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; M Charles, DO, EIS Officer, CDC. Editorial Note:This report highlights increased norovirus circulation in the United States. Noroviruses are the most common cause of gastroenteritis in the United States and cause an estimated 23 million cases of AGE annually (1). Although attention has been drawn recently to outbreaks of norovirus on cruise ships, an estimated 60%--80% of all outbreaks of AGE occur on land (4). In addition, although many reports have focused on foodborne transmission of noroviruses (7), this and other recent reports highlight the potential of norovirus to cause large outbreaks in institutional settings through nonfoodborne modes of transmission (4,5,8). Anecdotal reports from other state health departments throughout the United States also are consistent with recent increased activity of norovirus within institutional and closed settings. The cause of the increase in norovirus activity is unclear, although it is probably associated with an increase in community incidence of norovirus infection, as suggested in NYC and New Hampshire. Outbreaks of norovirus disease in closed settings have been documented, particularly during the winter (8,9). Since July 2002, a total of 41% of outbreaks in which strains were characterized genetically at CDC were associated with a single, newly identified strain of norovirus. The strain was found in various settings and over a wide geographic distribution, and no common source of these outbreaks has been identified. The finding of a predominant strain is unusual and contrasts with surveillance data from 1997--2000, which rarely detected identical strains from distinct outbreaks (4). However, data from 1995--1997 suggested the emergence of a globally common strain that accounted for 55% of all norovirus outbreaks investigated by CDC during that period (5). Like the Farmington Hills strain, the "common strain" of 1995--1997 was classified as a GII/4 strain. These strains have been associated previously with outbreaks in closed settings, and it is possible that this GII/4 predominant strain of norovirus has characteristics of infection that increase person-to-person transmissibility, such as an increased prevalence of vomiting (4). Characteristics of norovirus include a low infectious dose, relative stability in the environment, and spread through multiple modes of transmission (Box, which make norovirus outbreaks difficult to control (8,9). Measures to prevent spread should include emphasizing basic food and water sanitation measures and encouraging good hygiene, particularly appropriate hand washing techniques, disposal of waste and soiled materials, and disinfection. Development of more sensitive and specific RT-PCR detection methods and the increased use of nucleotide sequencing of detected strains (4,6) has enabled the identification of a common strain of norovirus and the possibility of linking outbreaks of norovirus disease throughout the United States and the world. However, no surveillance of nonfoodborne outbreaks of AGE exists in the United States (10). Development of improved surveillance systems to monitor endemic and epidemic norovirus disease is needed to understand modes of transmission and identify more specific control measures. CaliciNet is a database system under development that collects molecular and epidemiologic data from outbreaks of norovirus throughout the United States (CDC, unpublished data, 2002). Efforts to incorporate web-based reporting of nonfoodborne outbreaks of AGE by states are under way. CDC encourages local and state health departments to test for noroviruses when investigating outbreaks of suspected viral AGE. For assistance in testing for noroviruses and for strain characterization, local and state health departments should contact CDC's Viral Gastroenteritis Section, telephone 404-639-3577 or e-mail [email protected]. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
Page converted: 1/23/2003
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 1/23/2003