|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
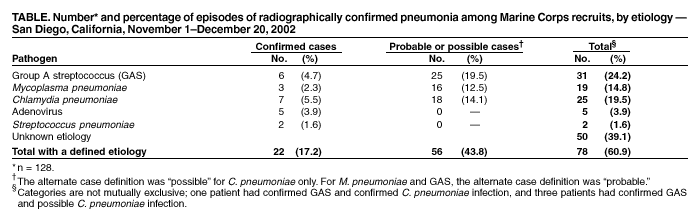
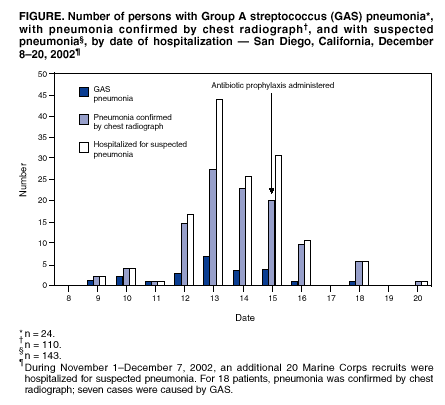
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreak of Group A Streptococcal Pneumonia Among Marine Corps Recruits --- California, November 1--December 20, 2002During November 1--December 20, 2002, a total of 163 Marine Corps personnel from the Marine Corps Recruit Depot (MCRD) in San Diego, California, including 160 new recruits, were admitted to the Naval Medical Center San Diego (NMCSD) for possible pneumonia. For 128 (79%) patients, pneumonia was confirmed by chest radiograph; of these 128 cases, 31 (24%) were definitely or probably caused by group A streptococci (GAS). This is the first outbreak of serious GAS-associated illness at a San Diego military training facility since the 1987 outbreak of rheumatic fever (1) and the largest outbreak of GAS pneumonia in the United States since 1968 (2). This report summarizes the results of the investigation of this outbreak, which indicate that GAS infection can occur among military recruit populations despite routine chemoprophylaxis administered to incoming recruits. Instituting routine surveillance for noninvasive GAS disease in military training facilities might prevent future invasive GAS outbreaks. All patients with radiographically confirmed pneumonia were tested by sputum, blood, and throat cultures; Mycoplasma pneumoniae IgM (ETI-MP enzyme-linked immunosorbent assay [ELISA], Diasorin, Inc.) and IgG (ELISA, Wampole); Chlamydia pneumoniae IgM and IgG (microimmuno-fluorescence, Focus Technologies); rhinoprobe direct fluorescent antibody for respiratory syncytial virus, adenovirus, influenzae, and parainfluenzae; urine Legionella antigen test; urine Streptococcus pneumoniae antigen test; and an antistreptolysin O (ASO) titer. Available GAS isolates underwent emm-typing through sequencing of the 5' emm variable region and antimicrobial susceptibility testing by broth microdilution and E-test. All case definitions required radiographic confirmation of pneumonia in a marine recruit hospitalized with acute respiratory illness (ARI) during the outbreak period. A confirmed case of GAS pneumonia required a blood or pleural fluid culture that was positive for GAS. A probable case of GAS pneumonia required a positive throat or sputum culture for GAS or an ASO titer of >250 Todd units in the absence of another identified etiologic agent. A confirmed case of M. pneumoniae pneumonia required IgG seroconversion, and a probable case required a positive IgM. A confirmed case of C. pneumoniae required a fourfold rise in IgG or an IgM titer of >16, and a possible case required an IgG titer of >512. A total of 128 male recruits aged 18--33 years (median: 20 years) had radiographically confirmed pneumonia; 110 (86%) were white non-Hispanics, 14 (11%) were white Hispanics, and four (3%) were members of other racial/ethnic groups. All recruits were previously healthy and were seronegative for human immunodeficiency virus. Of the 128 recruits with confirmed pneumonia, 66 (52%) had multilobar involvement, and 29 (23%) had a pleural effusion, including five (4%) with an empyema. GAS was identified in 31 (24%) pneumonia episodes (six confirmed and 25 probable GAS cases), resulting in a GAS pneumonia attack rate of 0.7% among the approximately 4,500 recruits present at the training facility during November 1--December 20. An etiologic agent could be established for 47 (48%) of 97 remaining pneumonia episodes and for 78 (61%) of the pneumonia episodes overall (Table). Multiple etiologies were identified for several pneumonia cases; one patient had confirmed GAS and confirmed C. pneumoniae infections, and three patients had confirmed GAS and possible C. pneumoniae. Sputum or throat cultures were positive for GAS or the patient had an ASO of >250 Todd units in two (29%) of the seven confirmed and five (28%) of the 18 possible C. pneumoniae cases, one (33%) of the three confirmed and nine (56%) of the 16 probable M. pneumoniae cases, and one (20%) of the five adenovirus cases. Symptoms reported by the 31 recruits with GAS pneumonia included cough (29 [94%]), fever (20 [65%]), sore throat (19 [61%]), pleuritic chest pain (15 [48%]), dyspnea (14 [45%]), chills (nine [29%]), and exanthem (two [7%]). The mean ASO titer for GAS pneumonia cases was 997 Todd units (range: <25-->4,800) compared with 249 for non-GAS cases (p = 0.03). Those with GAS were more likely to have an empyema (16% versus 0%; p = 0.005) and had a longer mean hospital stay (5.4 versus 2.4 days; p = 0.03) than those with non-GAS pneumonia. Two patients with GAS had streptococcal toxic shock syndrome (TSS) and required intensive care management. All recruits with pneumonia were treated successfully with ceftriaxone and either levofloxacin or azithromycin; clindamycin also was administered to those with TSS. One marine recruit died of purpura fulminans caused by Neisseria meningitidis serogroup C during the outbreak period. All GAS isolates were identified as emm type 3. In addition, all GAS isolates were susceptible to all 15 antibiotics tested, including penicillin, erythromycin, and azithromycin. Before the outbreak, recruits had received intramuscular benzathine penicillin on the day of arrival at MCRD and 28 days later (or oral erythromycin twice daily) as prophylaxis against streptococcal disease. Of the 31 recruits with GAS pneumonia, 27 (87%) were hospitalized with suspected pneumonia >21 days after the last dose of penicillin was administered. The epidemic was halted by re-administration of antibiotic prophylaxis to all 4,500 recruits at the facility on December 15 by using benzathine penicillin 1.2 million units intramuscularly; azithromycin 1 g was administered orally for those recruits who reported a penicillin allergy (Figure). Medical personnel from NMCSD, MCRD, and the Naval Health Research Center were involved in halting the outbreak. Reported by: NF Crum, MD, BR Hale, MD, DA Bradshaw, MD, JD Malone, MD, HM Chun, MD, WM Gill, MD, D Norton, MD, CT Lewis, MD, AA Truett, MD, C Beadle, MD, JL Town, MSN, MR Wallace, MD, Naval Medical Center; DJ Morris, MD, EK Yasumoto, MD, Marine Corps Recruit Depot; KL Russell, MD, Naval Health Research Center, San Diego, California. E Kaplan, MD, Univ of Minnesota Medical School, Minneapolis. C Van Beneden, MD, Div of Bacterial and Mycotic Diseases, National Center for Infectious Diseases; R Gorwitz, MD, EIS Officer, CDC. Editorial Note:Outbreaks of ARI, including pneumonia, among military trainees are well documented (3,4). Factors that might contribute to increased ARI susceptibility in this population include the rapid gathering of persons from across the country into crowded living and working quarters, which exposes nonimmune persons to several pathogens, and the physical and psychological stressors of training. Disease prevention efforts include immunoprophylaxis (e.g., pneumococcal, meningococcal, and influenza vaccinations) and chemoprophylaxis (e.g., penicillin prophylaxis for streptococcal infections) administered to incoming recruits (3) and ongoing surveillance for ARI (4). A leading cause of bacterial ARI among military recruits is S. pyogenes or GAS, which manifests as outbreaks of GAS pharyngitis, acute rheumatic fever, and pneumonia (3). This outbreak involved the circulation of a single GAS serotype and probably evolved from the introduction of this strain into a population of recruits lacking type-specific immunity. Streptococcal emm type 3 (corresponding to M type 3) is one of the most common serotypes associated with invasive GAS disease in the United States (5,6) and has been associated frequently, along with M types 1, 5, and 18, with outbreaks among U.S. military recruits (3). Population-based surveillance for all invasive GAS infections in nine disparate locations in the United States indicated that pneumonia accounted for 11%--14% of reported cases and was the third most common syndrome after invasive cutaneous or soft tissue infections and bacteremia without a known source (5,6). Among the civilian population, outbreaks of GAS pneumonia are rare. A higher baseline rate of invasive and noninvasive GAS disease and a potential to delay seeking medical treatment for minor illness (including pharyngitis) among military recruit populations might account for this difference. Several pathogens were identified as the potential source of pneumonia among the 78 (61%) pneumonia episodes for which a causative agent could be identified, and several pneumonia patients had dual diagnoses. Whether this represents a true concurrent increase in multiple respiratory pathogens or is an artifact of the diagnostic testing methods used is uncertain. The findings in this report are subject to at least three limitations. First, a definitive diagnosis of GAS pneumonia is difficult. Blood cultures frequently are negative in GAS pneumonia (2); therefore, a confirmed diagnosis might not be possible unless pleural fluid is obtained. Second, because positive throat or sputum cultures can represent simple GAS pharyngitis or asymptomatic carriage of the organism, the specificity of these cultures for diagnosis of GAS pneumonia is low. Rising ASO titers might distinguish between GAS carriage and infection but are not specific for invasive GAS disease (7). Finally, diagnosing M. pneumoniae and C. pneumoniae infections by serology alone can be problematic, especially in the context of known GAS infections. Several serologic assays for M. pneumoniae are available commercially but vary in sensitivity and specificity (8). Although the microimmunofluorescence assay is considered the method of choice for serologic diagnosis of C. pneumoniae infection, interpretation of the results can be subjective. False positives can occur for M. pneumoniae and possibly for C. pneumoniae serologic assays in the presence of a nonspecific antibody response to GAS infection. Primary and secondary penicillin chemoprophylaxis for GAS infections is effective in military recruit populations and has been used intermittently since 1951 (3,4). Primary (i.e., tandem) prophylaxis is administered to all recruits shortly after their arrival at a training facility to prevent the introduction of GAS into this population, and secondary (i.e., mass) prophylaxis is provided concurrently to all recruits in a given facility to interrupt established disease transmission. Oral erythromycin or azithromycin prophylaxis is used to prevent infection among recruits who are allergic to penicillin. The reason that primary prophylaxis failed in this circumstance is unclear. Possible explanations include failure to achieve adequate serum levels of penicillin (9), waning protection as serum levels declined before the second scheduled dose of penicillin was administered on training day 28, and lack of compliance with oral erythromycin among penicillin-allergic recruits. Eradicating GAS carriage is difficult even with appropriate doses of penicillin and in the absence of penicillin resistance (10). Early diagnosis and management of GAS infections might prevent the development of suppurative complications. Routine surveillance for noninvasive GAS disease was initiated recently at MCRD to identify breakthrough GAS infections and prevent outbreaks of GAS disease. Institution of routine surveillance for noninvasive GAS disease also might be useful for other military training facilities. Acknowledgments This report is based on assistance provided by W MacAllister, J Christensen, Naval Medical Center San Diego, California, and by R Besser, MD, R Facklam, PhD, B Fields, PhD, D Talkington, PhD, WL Thacker, MS, and ML Tondella, PhD, Div of Bacterial and Mycotic Diseases, National Center for Infectious Diseases, CDC. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
Page converted: 2/13/2003
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 2/13/2003