|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
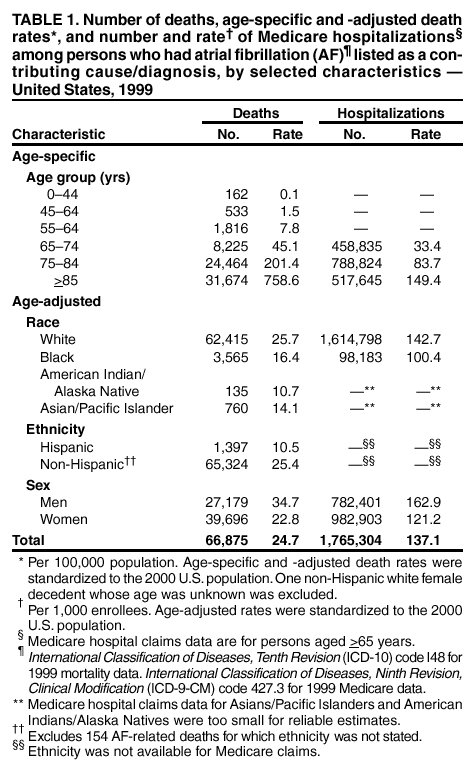
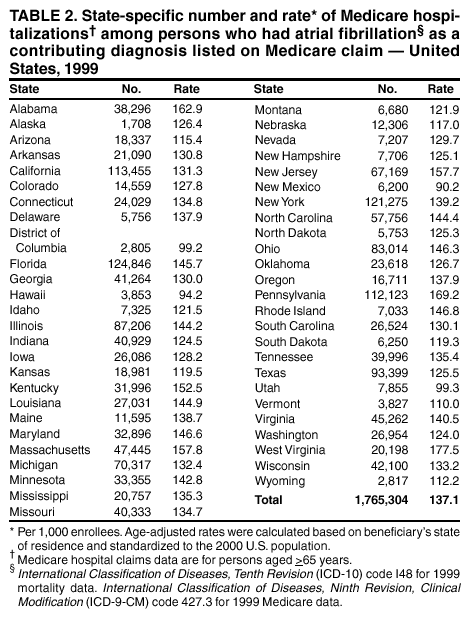
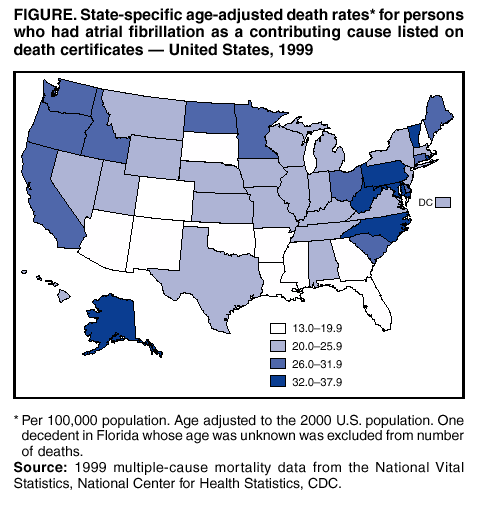
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Public Health and Aging: Atrial Fibrillation as a Contributing Cause of Death and Medicare Hospitalization --- United States, 1999Stroke is the leading cause in the United States of serious long-term disability and the third leading cause of death. One of the major risk factors for stroke is atrial fibrillation (AF), a common cardiac disorder characterized by cardiac arrhythmia and the absence of coordinated contractions, which increases the risk for blood stasis, clot formation, and embolic stroke. AF affects approximately 2.2 million adults in the United States (1,2) and is the most common sustained heart rhythm disturbance observed in clinical practice (3). The rate of AF increases with age, from <1% among persons aged <60 years to approximately 10% among persons aged >80 years (4). The frequency with which AF is reported on death certificates as a contributing cause of death has increased since 1980 (5). To assess the burden of AF-related deaths and hospitalizations among U.S. residents, CDC analyzed national and state multiple-cause mortality statistics and Medicare hospital claims for persons with AF in 1999 (the latest year for which data were available) for the 50 states and the District of Columbia. The findings indicate that AF as a contributing cause of death and hospitalization affects primarily persons aged >75 years and that death and hospitalization rates vary by state. Public and medical education are needed to prevent and reduce AF-related disability and death. National and state multiple-cause mortality statistics were obtained from death certificates in state vital statistics offices and compiled by CDC. AF-related deaths are those for which the contributing cause of death* (any one of the 20 possible conditions listed on the death certificate) listed by a physician or a coroner is classified as code I48 according to the International Classification of Diseases, Tenth Revision (ICD-10). Among decedents who had AF, the proportion of those who had an underlying cause of death listed as AF (ICD-10 I48), coronary heart disease (ICD-10 I20--I25), or stroke (ICD-10 I60--I69) also was assessed. Demographic data (age, sex, and race/ethnicity) on death certificates were reported by funeral directors or provided by family members of the decedent. The denominators for death rates were obtained from 1999 census records and included only U.S. residents. Medicare (Part A) hospital claims and enrollment records from the Medicare Provider Analysis and Review files were obtained from the Centers for Medicare and Medicaid Services. AF-related hospitalizations among Medicare enrollees aged >65 years were classified as code 427.3 according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) as one of six diagnoses on the hospital claims during 1999. The denominators for hospitalization rates were obtained from Medicare enrollment records and included enrollees aged >65 years who were entitled to Medicare Part A benefits on July 1, 1999 (excluding 15.7% of members with coverage from health maintenance organizations). Among persons hospitalized with AF, the proportion of those who had a primary hospital diagnosis of AF (ICD-9 427.3), coronary heart disease (ICD-9 410--414, 429.2), or stroke (ICD-9 430--434, 436--438) also was assessed. AF-related death rates for groups defined by age, sex, race/ethnicity, and state were determined by dividing the number of deaths by the population at risk (denominator) in each group. Rates of hospitalizations among Medicare enrollees aged >65 years with AF for each group were determined by dividing the number of hospitalizations by the population at risk (denominator) in the group. Age-adjusted death rates (per 100,000 population) and hospitalization rates (per 1,000 Medicare enrollees) were calculated by using the 2000 U.S. standard population (6). In 1999, a total of 66,875 deaths with AF as a contributing cause occurred, resulting in an age-adjusted death rate of 24.7 per 100,000 population. Of these deaths, 56,138 (84.0%) were among persons aged >75 years. The greatest proportion of these AF-related deaths occurred among persons aged >85 years (47.4%), followed by those aged 75--84 years (36.6%), aged 65--74 years (12.3%), and aged <65 years (3.7%). Age-specific death rates increased for successive age groups (Table 1). Age-adjusted death rates for AF were highest among whites (25.7) and blacks (16.4) and higher for men (34.7) than women (22.8). In 1999, for all decedents who had AF, the most common underlying causes of death were coronary heart disease (28.0%), AF (12.4%), and stroke (10.8%). In 1999, a total of 1,765,304 hospitalizations (137.1 per 1,000 Medicare enrollees) were reported among persons with AF in the Medicare population (Table 1). Rates increased among successive age groups. The rate of hospitalization among persons with AF was higher among whites (142.7) than among blacks (100.4). Although 55.7% of these hospitalizations were among women, men (162.9) had a higher rate of AF-related hospitalization than women (121.2). The most common diseases listed as the primary diagnosis for persons hospitalized with AF were congestive heart failure (11.8%), followed by AF (10.9%), coronary heart disease (9.9%), and stroke (4.9%). The state-specific age-adjusted death rates for AF ranged from 13.1 in Arizona to 37.4 in Maryland (Figure). The age-adjusted rate of hospitalizations among persons with AF ranged from 90.2 in New Mexico to 177.5 in West Virginia (Table 2). Reported by: C Ayala, PhD, WA Wattigney, MS, JB Croft, PhD, A Hyduk, MPH, GA Mensah, MD, Div of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion; H Davis, PhD, EIS Officer, CDC. Editorial Note:The findings in this report confirm that AF is a contributing cause of death among older persons, particularly those aged >75 years, and that state-specific AF-related death rates vary. These findings are consistent with other trends of AF-related deaths (5). Patterns in the rate of AF-related hospitalization among Medicare enrollees are similar to those for death rates. The high proportion of AF-related deaths and hospitalizations occurring among persons aged >75 years suggests that as the population ages, AF might be diagnosed more frequently. A cohort study of hospitalized Medicare patients indicated that medical costs were greater for patients with AF than for those without AF (7). In addition, effective therapies for AF reduced the risk for stroke by >70%. Patients who have coronary heart disease, hypertensive disease, or stroke diagnosed and who live longer might be at risk for AF if effective therapy is not maintained (8). Serious complications among patients with uncontrolled AF also can include congestive heart failure, myocardial infarction, and thrombotic stroke. Initial treatment of AF should be directed at controlling the ventricular rate with a calcium channel blocker, beta-blocker, or digitalis (3). Medical or electrical cardioversion to restore sinus rhythm is the next step in patients who remain in AF. Effective therapies in preventing stroke and cardiovascular complications include anticoagulation, heart rate control, conversion of AF to normal heart rhythm, and catheter-based and surgical interventions (3). Educating the public to recognize the signs of cardiac arrhythmia can help identify persons with AF. Persons can identify an irregular heartbeat by monitoring their wrist pulse for 1 minute. The irregularity of these beats is detected and the next beat cannot be predicted. Persons who identify the signs of cardiac arrhythmia should seek medical care to determine the presence of AF or other heart disorders. The Research Center for Stroke and Heart Disease (http://www.strokeheart.org), has initiated the educational campaign, "Take Your Pulse For Life." This initiative recommends that persons, particularly those aged >55 years, monitor their pulse for 1 minute the first day of every month. Assessing whether a patient has AF can be easy and inexpensive through using electrocardiography (ECG) (3); the availability of more advanced diagnostic tools, such as ECG monitoring, might contribute to AF diagnosis in persons suspected to have cardiac arrhythmia. Delay in diagnosis occurs when the rhythm has not been documented specifically and additional monitoring is necessary (3). All persons should know how to take a pulse for themselves or their family members. The findings in this report are subject to at least two limitations. First, data are subject to misclassification of race/ethnicity both in the population census and on death certificates, possibly resulting in overreporting among blacks and whites and underreporting among other racial/ethnic groups (9). Second, it was not possible to determine the accuracy of physician or administrative reporting, the validity of the ICD codes, or multiple hospitalizations on Medicare hospital claims. Because AF is one of the major treatable risk factors for stroke, prevention of AF through public and medical education for early identification and appropriate treatment should become an important focus of public health efforts to reduce stroke- related deaths and disability. Prevention efforts should include broad-based public health efforts to increase public awareness of AF and to foster timely and appropriate diagnostic evaluation and effective treatment from health-care providers. References
* Contributing cause of death was defined as the subsequent diagnosis considered with the cause of death, and underlying cause of death was defined as the primary diagnosis associated with the death.
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 2/20/2003 |
|||||||||
This page last reviewed 2/20/2003
|