|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
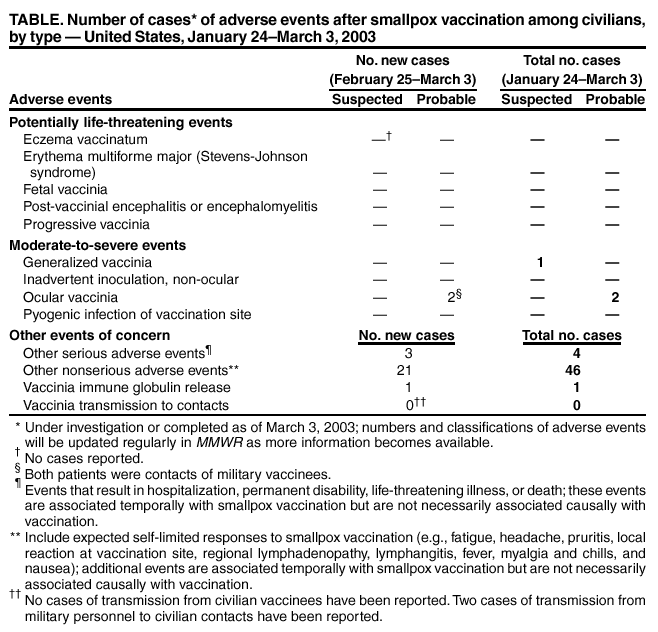
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Smallpox Vaccine Adverse Events Among Civilians --- United States, February 25--March 3, 2003During the civilian smallpox vaccination program, CDC, the Food and Drug Administration, and state health departments are conducting surveillance for vaccine-associated adverse events. In the first stage of the program, active surveillance is being conducted for potentially life-threatening, moderate-to-severe, and other serious adverse events and for vaccinia transmission to contacts of vaccinees (1) (Table). Nonserious events are reported through passive surveillance and are expected to be underreported. This report summarizes smallpox vaccine adverse events reported among civilians vaccinated as of February 28, 2003, and among contacts of vaccinees, received by CDC from the Vaccine Adverse Event Reporting System (VAERS) as of March 3. Potentially life-threatening and moderate-to-serious events are classified on the basis of evidence in support of the reported diagnoses. For probable cases, other causes are excluded, and supportive information is available. Events are classified as suspected if they have clinical features compatible with the diagnosis but either further investigation is required or additional investigation of the case did not provide supporting evidence for the diagnosis and did not identify an alternative diagnosis. CDC and state and local health departments also receive reports of other events that are associated temporally with smallpox vaccination. Reported adverse events are not necessarily associated with vaccination, and some or all of these events might be coincidental. During January 24--February 28, smallpox vaccine was administered to 12,690 civilian health-care and public health workers in 45 jurisdictions. No potentially life-threatening adverse events of a type known previously to be caused by smallpox vaccination have been reported as of March 3. Two moderate-to-severe adverse events were reported (Table). Both were probable cases of ocular vaccinia, and both were traced to contact with military personnel who received smallpox vaccine. A woman aged 26 years slept in the same bed several times a week over a 3-week period with a military vaccinee beginning shortly after he received smallpox vaccine; he was reported often not to have kept his vaccination site covered. The woman became ill with swelling, pain, and discharge from the right eye, which progressed over the course of 1 week to swelling of the entire right side of the face, difficulty opening and impaired vision in the right eye, and increased exudate, despite treatment with antibacterial eyedrops. On February 22, she was hospitalized. Ophthalmologic examination revealed severe right scleral injection and chemosis, a small pustule at the right palpebral lower lid margin, and tender right preauricular and submandibular adenopathy but found no evidence of keratitis, iritis, or periocular lesions. Orbital computerized tomography scan was consistent with preseptal cellulitis without infection of the globe. The patient's preseptal cellulitis improved within 24 hours after treatment with intravenous antibiotics, and she was discharged on February 25. The following day, the patient was readmitted with persistent right blepharoconjunctivitis. Preliminary viral cultures of conjunctival fluid revealed cytopathic effect consistent with viral infection, and a direct fluorescent antibody test was positive for vaccinia. The patient improved within 24 hours after treatment with trifluridine eyedrops and a single dose of intravenous vaccinia immune globulin. She was discharged on February 28. The viral culture material and a swab sample from the patient's eye were sent to CDC and tested positive for vaccinia DNA by real-time polymerase chain reaction (PCR). On February 14, a woman aged 18 years with no history of smallpox vaccination handled the bandage of a military vaccinee. The woman had a pustular skin lesion (size: 1.5 cm) with a small satellite lesion on her right forearm 3 days after this contact and a second pustular lesion on the back of her upper right arm 5 days after contact, followed by irritation and swelling in her right eye 8 days after contact. The patient first sought medical attention 11 days after the contact and had a skin condition and bacterial conjunctivitis diagnosed, which were treated with an oral antibiotic; 14 days after contact, she was noted to have two small pustular lesions on her right eyelid and had blepharoconjunctivitis diagnosed. She had marked improvement within 24 hours after initiating treatment with trifluridine eye drops. Specimens taken from eye and skin lesions demonstrated vaccinia virus based on PCR. Three other serious adverse events were reported (Table). One case involved headache and dizziness; although headache has been reported after smallpox vaccination, the casual role of smallpox vaccine in this case is unknown. The other two events (cholecystitis and hypertension) are not known to be associated causally with smallpox vaccination. A woman aged 38 years had headache and dizziness 5 days after smallpox vaccination; 6 days later, after the symptoms had increased in intensity, she was admitted to a hospital for evaluation. A neurologist observed no change in mental status or other neurologic deficits; an MRI brain scan showed no abnormalities. The patient's symptoms improved, and she was discharged 2 days later. A man aged 46 years with a history of hypertension was hospitalized 1 day after vaccination with hypertension (blood pressure: approximately 230/120) and severe headache. The patient was treated with antihypertensive medications and was discharged after 1 day. A woman aged 51 years had onset of chest discomfort, shortness of breath, and nausea 2 days after vaccination. The patient had cholelithiasis with ductal blockage diagnosed and had a cholecystectomy; she was discharged after 3 days. Among the 46 vaccinees with reported other nonserious adverse events during January 24--March 3 (Table), the most common signs and symptoms were fever (n = 11), pruritus (n = 11), rash (n = 10), and pain (n = seven). All of these commonly reported events are consistent with mild expected reactions following receipt of smallpox vaccine. Some vaccinees reported multiple signs and symptoms. Surveillance for adverse events during the civilian smallpox vaccination program is ongoing; regular surveillance reports will be published in MMWR. Reported by: Smallpox Vaccine Adverse Events coordinators. National Center for Infectious Diseases; National Immunization Program, CDC. Editorial Note:This report highlights the importance of proper vaccination site care in preventing contact transmission of vaccinia virus and the need for vacinees and unvaccinated persons who have contact with vaccinees to protect against contact transmission (2). Vaccinees who do not work in health-care settings should cover the vaccination site with a gauze bandage that is secured by first-aid adhesive tape and should change the bandage frequently (i.e., every 1--3 days). Vaccinees should keep the vaccination site dry, cover it with a waterproof bandage during bathing, and change back to a gauze bandage after bathing. Gauze bandages should be changed whenever they become wet. As an added precaution, vaccinees should wear a long-sleeved shirt that covers the vaccination site, particularly in situations involving close physical contact. Vaccinees should practice consistent hand hygiene by washing thoroughly with antimicrobial soap and water or with an approved alcohol-based hand-rub (i.e., one that contains >60% alcohol) after any contact with the vaccination site or with materials that have come into contact with the site, including bandages, clothing, towels, and sheets. Contaminated bandages and scabs from the vaccination site should be placed in a sealed plastic bag and discarded. Vaccinees should keep a separate laundry hamper for clothing, towels, sheets, and other items that might have come in direct contact with the vaccination site or with drainage from the site; these items should be washed by using hot water with detergent and/or bleach. Contacts of vaccinees should not touch the vaccine site or any materials that might be contaminated with vaccine virus, including bandages, clothing, towels, or sheets. Contacts who touch any potentially contaminated materials inadvertently should wash their hands immediately. Vaccinated persons and their contacts who share a bed should be certain that the vaccination site is covered with a bandage and shirt sleeve. References
Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 3/6/2003 |
|||||||||
This page last reviewed 3/6/2003
|