|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
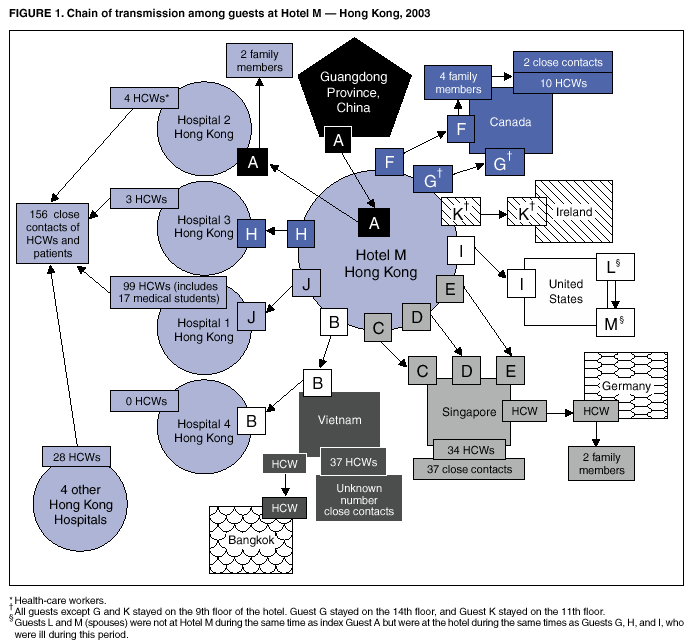
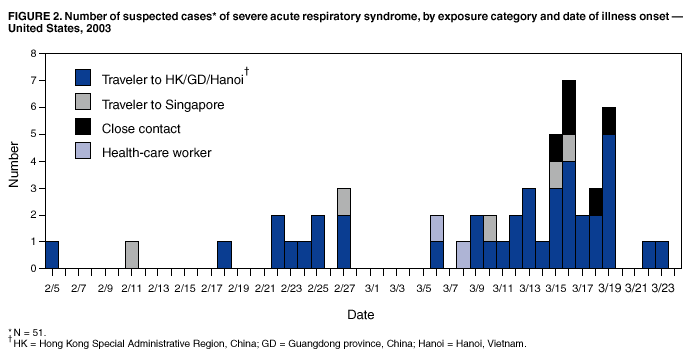
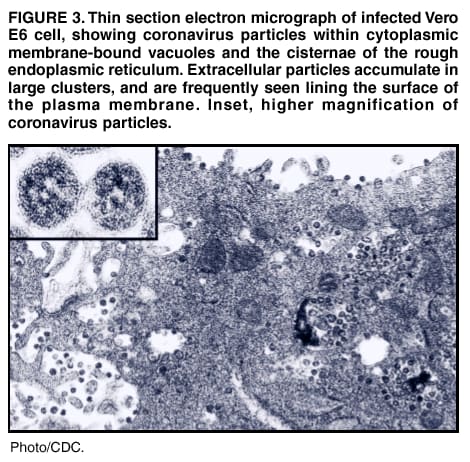
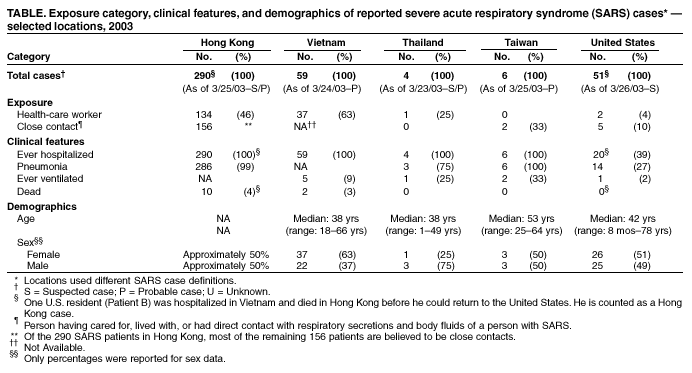
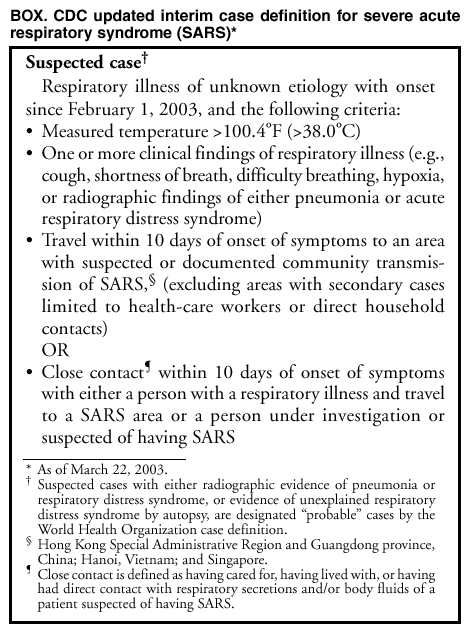
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Outbreak of Severe Acute Respiratory Syndrome --- Worldwide, 2003Please note: An erratum has been published for this article. To view the erratum, please click here. CDC continues to support the World Health Organization (WHO) in the investigation of a multicountry outbreak of unexplained atypical pneumonia referred to as severe acute respiratory syndrome (SARS) (1). This report includes summaries of the epidemiologic investigations and public health responses in several affected locations where CDC is collaborating with international and national health authorities. This report also describes an unusual cluster of cases associated with a hotel in Hong Kong and identifies the potential etiologic agent of SARS. Epidemiologic and laboratory investigations of SARS are ongoing. As of March 26, a total of 1,323 suspected and/or probable SARS cases have been reported to WHO from 14 locations (2), using the WHO case definition or country-specific variations* (3). These reported SARS cases include 49 deaths (case-fatality proportion: 4%). The Chinese authorities have reported 792 suspected/probable cases, including 31 deaths, which occurred in Guangdong province during November 16, 2002--February 28, 2003. CDC is assisting in epidemiologic investigations of cases in Hong Kong, Vietnam, Taiwan, and Thailand. CDC also is conducting surveillance and prevention activities in the United States. Hong Kong. As of March 25, the Hong Kong Department of Health (DH) reported 290 suspected and probable SARS cases. Beginning on March 11, an increase in acute pneumonia cases among health-care workers (HCWs) at hospital 1 in Hong Kong was reported to DH. Epidemiologic investigation has linked these cases to an index patient (Patient J) who visited a friend in hotel M in late February, became ill a few days later, and was admitted to hospital 1 on March 4 (Figure 1). Patient J visited hotel M while patient A, an ill visitor from Guangdong province, was staying there. As of March 25, a cluster of 13 persons with suspected/probable SARS are known to have stayed at hotel M (Figure 1). The index patient (patient A) had onset of symptoms on February 15. He traveled from Guangdong province to Hong Kong to visit family and stayed on the ninth floor of the hotel on February 21. He was admitted to hospital 2 on February 22 and died the next day. Four HCWs and two of his family members subsequently became ill; one family member died. Of the 12 other patients linked to hotel M, 10 were in the hotel the same day as the index patient; the other two patients (patients L and M) stayed in the hotel during the time that three other symptomatic patients were guests in the hotel. Nine of the 13 patients, including patient A, stayed on the ninth floor; one stayed on the 14th floor; one stayed on the 11th floor; and two stayed on both the ninth and 14th floors. Epidemiologic investigations have identified patients from this cluster as index patients in subsequent clusters in Hong Kong and other areas. Patient B is the index patient for the outbreak in Hanoi involving 59 HCWs and close contacts and also is linked to one case in Thailand. Patients C, D, and E are associated with 70 cases in Singapore and three cases in Germany. Patient F is linked with a cluster of 16 other cases in Toronto (4). Patients H and J are linked with outbreaks among HCWs in other hospitals in Hong Kong. Patient L appears to have become infected during his stay at hotel M, with subsequent transmission to his wife, patient M. As of March 25, six hospitals and one clinic in Hong Kong have reported nosocomial transmission to HCWs following admission of persons with SARS. The suspected index patients of three of the seven nosocomial clusters reported in Hong Kong have been associated with hotel M (Figure 1). Hong Kong health authorities have implemented enhanced infection-control procedures in all hospitals in Hong Kong, including more stringent barrier and respiratory protection for HCWs, at least daily environmental disinfection of affected wards, and cohorting of SARS patients. New cases among HCWs have declined following implementation of these new guidelines. However, new cases continue to be reported, predominantly among close contacts† of known patients. Vietnam. As of March 24, the Vietnamese Ministry of Health in Hanoi has reported 59 probable SARS cases (Table). The probable index patient (patient B) (Figure 1) was an Asian-American businessman aged 47 years who had visited Hong Kong before traveling to Hanoi. During his visit to Hong Kong, he had stayed at hotel M on the same floor, and during the same time, as patient A. Patient B became ill after arrival in Hanoi on February 23 and was hospitalized with lower respiratory symptoms on February 26. On March 2, he was placed on mechanical ventilation. On March 5, he was medically evacuated to a hospital in Hong Kong and died on March 12. By March 5, secondary probable SARS cases were identified among HCWs in Hanoi. All probable SARS cases reported as of March 24 in Hanoi have been linked through primary or secondary exposure to the same hospital. Two patients who were exposed to hospitalized SARS patients traveled subsequently to Thailand and France and are not included in these numbers. The government of Vietnam has implemented control activities in Hanoi and throughout the country, including daily follow-up of contacts of probable SARS cases and community surveillance for suspected SARS cases. Infection-control practices to prevent nosocomial transmission have been implemented at Hanoi hospitals with probable SARS cases. Nosocomial cases have decreased since the initial peak of cases linked to exposure to the index patient. Thailand. As of March 23, the Ministry of Public Health in Thailand has reported four suspected/probable cases (Table). Dates of illness onset ranged from March 11 to March 18. Of these four ill persons, three reported travel to Hong Kong during the week before illness onset; the other person is a physician who cared for SARS patients in Hanoi. Thailand has begun to implement hospital infection control procedures on the presumption of airborne spread. Gowns, gloves, and N-95 masks are widely available in Thailand. As of March 26, surveillance has not documented spread of infection to HCWs. However, one HCW from Thailand became infected while investigating the outbreak in Hanoi. Taiwan. As of March 25, the Taiwan Department of Health has reported six probable cases (Table). Dates of illness onset ranged from February 25 to March 17. Of these six ill persons, four reported travel to Guangdong province and Hong Kong during the week before illness onset; none of them had stayed at hotel M. The other two cases occurred in family members of the first patient. Two patients required mechanical ventilation but have improved clinically. On the basis of presumed airborne spread of SARS, Taiwan has aggressively implemented and monitored strict infection-control procedures. Negative pressure rooms and N-95 respirators are uniformly available for hospitalized patients. Active surveillance has not identified nosocomial transmission. Epidemiologic studies are under way to determine specific risk factors for transmission. United States. As of March 26, CDC has received 51 reports of suspected SARS cases from 21 states (Table), identified using the CDC updated interim case definition (Box (Figure 2). The first suspected case was identified on March 15, in a man aged 53 years who traveled to Singapore and became ill on March 10. Four clusters of suspected cases have been identified, three of which involved a traveler who had visited Southeast Asia (including Guangdong province, Hong Kong, or Vietnam) and a single family contact. One of these clusters involved suspected cases in patients L and M (Figure 1), who had stayed together at hotel M during March 1--6, when other hotel guests were symptomatic. Patient L became sick on March 13 after returning to the United States. His wife, patient M, became ill several days after the onset of her husband's symptoms, suggesting secondary transmission. Three patients in the United States with suspected SARS (patients I, L, and M) reported staying at hotel M when other persons staying in the hotel were symptomatic. The fourth cluster began with a suspected case in a person who traveled in Guangdong province and Hong Kong. Two HCWs subsequently became ill at the U.S. hospital where this patient was admitted. Laboratory investigations. On March 24, CDC announced that laboratory analysis had identified a previously unrecognized coronavirus in patients with suspected or probable SARS. The new coronavirus was isolated in Vero E6 cells from clinical specimens of two patients in Thailand and Hong Kong with suspected SARS. The isolate was identified initially as a coronavirus by electron microscopy (EM) (Figure 3). The identity was corroborated by results of immunostaining, indirect immunofluorescence antibody (IFA) assays, and reverse transcriptase-polymerase chain reaction (RT-PCR) with sequencing of a segment of the polymerase gene. IFA testing of sera and RT-PCR analysis of clinical specimens from six other SARS cases were positive for the new coronavirus. Coronavirus particles also were identified by EM in cells obtained by bronchial lavage from a patient with SARS. Sequence analysis suggests that this new agent is distinct from other known coronaviruses. Other laboratories collaborating in the WHO-led investigation have found similar results and also have isolated a different virus, human metapneumovirus, from some patients with suspected SARS. Information is insufficient to determine what roles these two viruses might play in the etiology of SARS. Reported by: T Tsang, T Lai-Yin, L Pak-Yin, M Lee, Dept of Health, Hong Kong. J-S Wu, Y-C Wu, I-H Chiang, K-T Chen, K-H Hsu, T-J Chen, Taiwan Center for Disease Control; L-T Lee, S-J Twu, Taiwan Dept of Health, Taiwan. S Chunsuttiwat, P Sawanpanyalert, K Ungchusak, A Chaovavanich, Ministry of Public Health, Thailand. Ministry of Health of Vietnam, WHO SARS Investigative Team, Vietnam. CDC SARS Investigative Team, SL Roy, MD, EIS Officer, CDC. Editorial Note:Cases of SARS continue to be reported from around the world. These cases are linked primarily to areas with ongoing transmission, with some reports of secondary local transmission. Transmission has been reported in Guangdong Province, Hong Kong, Singapore, and Hanoi. In Canada, transmission appears to be limited to a well-defined population of HCWs and close contacts. In Taiwan, limited transmission has occurred to family members but not to HCWs. Chinese authorities have updated the number of cases in Guangdong province and confirmed ongoing disease activity. The numbers of reported cases in Canada, Singapore, and the United States also continue to increase (2). Transmission in hospitals and households continues to occur. In addition, reports have been received of possible transmission on ships and planes and in offices. On the basis of available information, country-specific efforts to limit and halt transmission have included enhancing surveillance, improving infection-control measures in hospitals and homes, selectively closing hospitals and schools, furloughing hospital staff, issuing travel advisories, restricting movement of patients with suspected SARS, and establishing quarantines of exposed persons. In the United States, CDC has issued travel advisories and developed infection-control guidelines; efforts have been focused on rapid identification and early isolation of symptomatic persons whose illnesses meet the CDC case definition. The summary of the demographic, clinical, and transmission patterns from the reported areas documents some disparities in case-fatality proportion with pneumonia, and ease of transmission. The data also highlight gaps in knowledge about the epidemiology of this new syndrome. Some differences probably reflect concomitant differences in case definition and surveillance methodologies. However, because of the nonspecific case definition, all reported cases might not represent a single clinical entity. Confirmation of the etiology and development of a diagnostic test should help to resolve these discrepancies. Although the mechanism of SARS transmission remains unclear, on the basis of the reported exposures for the majority of cases (i.e., household contacts and HCWs), droplet and contact transmission appear to be the predominant modes. The cases in the hotel M cluster and certain hospital clusters involving seriously ill patients suggest airborne or fomite transmission. Therefore, infection-control recommendations should include precautions to prevent airborne, droplet, and contact transmission. With the introduction of these control measures, decreases in the reported incidence of SARS have been reported in Hong Kong. Although the etiologic agent has not been confirmed, laboratory data indicate that a metapneumovirus or a coronavirus are possible agents. Infection with a metapneumovirus, (i.e., enveloped, single-stranded RNA virus) has been associated previously with respiratory disease with much less frequent occurrence of severe disease than SARS. Coronaviruses are enveloped, single-stranded RNA viruses that infect both humans and animals (5). The known human coronaviruses can cause serious infections of the lower respiratory tract in children and adults and necrotizing enterocolitis in newborns (5,6). Coronaviruses are able to survive on environmental surfaces for up to 3 hours (6). Coronaviruses might be transmitted person-to-person by droplets, hand contamination, fomites, and small particle aerosols (7). Clinicians evaluating suspected cases should use standard precautions (e.g., hand hygiene) together with airborne (e.g., N-95 respirator) and contact (e.g., gowns and gloves) precautions (8). Until the mode of transmission has been defined more precisely, eye protection also should be worn for all patient contact. As more clinical and epidemiologic information becomes available, interim recommendations will be updated. The international spread of disease underscores the need for strong global public health systems, robust health service infrastructures, and expertise that can be mobilized quickly across national boundaries to mirror disease movements. The Institute of Medicine has recently issued recommendations for invigorating the response to emerging infectious diseases that reflect these needs, including the development of a comprehensive system of surveillance for global infectious diseases, the enhancement of disease reporting, the development of diagnostic tests, and the formulation and distribution of guidelines on diagnosis (9). References
* WHO defines (3) a suspected case as an illness that occurs in a person presenting after February 1, 2003, with a history of high fever (>100.4 oF [ >38 oC]); one or more respiratory symptoms, including cough, shortness of breath, and difficulty breathing; and close contact within 10 days of symptoms onset with a person in whom SARS has been diagnosed and/or a history of travel within 10 days of onset of symptoms to an area with reported foci of SARS transmission. WHO defines a probable case as a suspected case of illness that occurs in a person with either 1) chest radiograph findings of pneumonia or respiratory distress syndrome (RDS) or 2) unexplained respiratory illness resulting in death, with autopsy examination demonstrating pathology of RDS but no identifiable cause. † Persons who have cared for, lived with, or had direct contact with respiratory secretions and body fluids of a person with SARS.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 3/27/2003 |
|||||||||
This page last reviewed 3/27/2003
|