|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
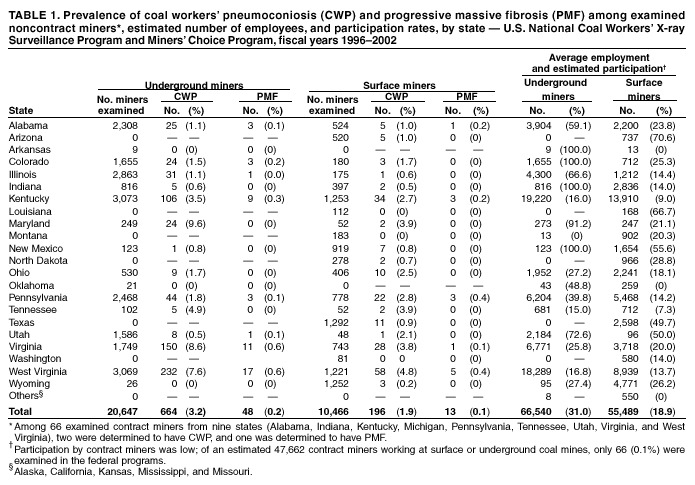
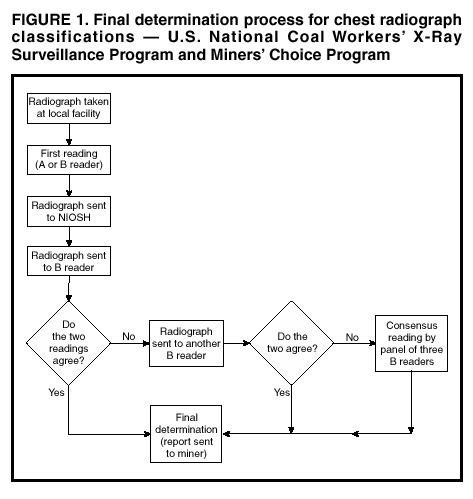
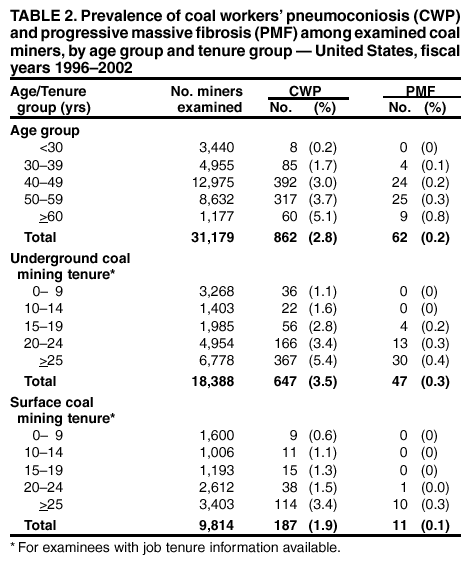
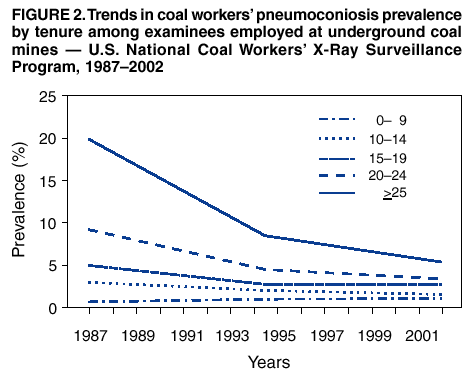
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Pneumoconiosis Prevalence Among Working Coal Miners Examined in Federal Chest Radiograph Surveillance Programs --- United States, 1996--2002Coal workers' pneumoconiosis (CWP) is a chronic lung disease caused by inhalation of coal mine dust. To characterize the prevalence of CWP, the National Institute for Occupational Safety and Health (NIOSH) analyzed recent radiographic information from the U.S. National Coal Workers' X-ray Surveillance Program (CWXSP). Established under the Federal Coal Mine Health and Safety Act of 1969 (1), CWXSP is administered by NIOSH under federal regulations (2). NIOSH is responsible for approving coal miner examination plans, submitted approximately every 5 years by companies that operate underground coal mines. This report summarizes the results of the analysis, which indicate that the overall prevalence of CWP among participating miners continues to decline; however, new cases are occurring among miners who have worked exclusively under current dust exposure limits. An evaluation of the mining conditions that have resulted in these cases is underway. Federal regulations specify that companies offer underground coal miners a chest radiograph at first employment and every 5 years thereafter while employed. Periodic radiographs that use a specified radiographic technique are offered during a 6-month examination period at NIOSH-approved health facilities. During October 1, 1999--September 30, 2002, NIOSH collaborated with the Mine Safety and Health Administration (MSHA) to accept films from MSHA's new Miners' Choice Program (MCP) for classification by using CWXSP procedures. Operating independently of coal mine operators, MCP ran concurrently with CWXSP and encouraged miners to undergo radiographic examination. MCP participants were miners from 586 surface coal mines, which are not required or encouraged to participate in CWXSP, and from 444 underground coal mines. Coal miner chest radiographs taken under these programs are classified by using the 1980 International Labour Office (ILO) International Classification of Radiographs of Pneumoconioses (3). To ensure proficiency in classification, NIOSH has established a two-tier system for designation of radiograph readers. "A" readers have completed a training course or have otherwise demonstrated competence in the use of the ILO Classification, and "B" readers have successfully completed a certification examination and must be recertified every 4 years (4). A final determination of the classification of each radiograph is made by using a standardized process and requires agreement between at least two readers, only one of whom may be an "A" reader, about both the presence and severity of apparent dust-related abnormalities (Figure 1) (2). An identification of CWP requires reader agreement that small pneumoconiotic opacities are present at an ILO profusion category of >1/0. An identification of progressive massive fibrosis (PMF), an advanced form of CWP, requires reader agreement on the presence of large pneumoconiotic opacities. During October 1, 1995--September 30, 2002, CWXSP and MCP received 35,983 readable chest films for 31,179 miners at 1,439 mines in 23 states. The crude prevalence of CWP among all examinees was 2.8% (862 cases), and the corresponding prevalence of PMF was 0.2% (62 cases). CWP prevalences among examinees who were noncontract employees at surface mines, noncontract employees at underground mines, and contract* miners were 1.9%, 3.2%, and 3.0%, respectively. Among the 16 states with underground noncontract miner examinees, CWP prevalences ranged from zero to 9.6%, and corresponding PMF prevalences ranged from zero to 0.6% (Table 1). Examinees from larger mines (>50 employees) had a lower prevalence of pneumoconiosis than those from smaller mines (2.0% versus 5.6% for CWP [p<0.0001], and 0.1% versus 0.5% for PMF [p<0.0001]). For all age groups, the prevalences of CWP and PMF increased with age (Table 2). Information about tenure in coal mining was available for 28,253 miners. For underground miners of all tenures (n = 18,388), CWP and PMF prevalences increased with underground mining tenure (Table 2). Corresponding tenure-specific prevalences among surface miners (n = 9,793) similarly increased with surface mining tenure. Participation rates were estimated by using the number of coal miners for whom radiographs were taken and the average number of coal miners employed during the same period, based on quarterly employment figures obtained from MSHA. Estimated participation rates were 25.5% for noncontract miners and 0.1% for contract miners and varied substantially by state (Table 1). Participation was higher among miners who worked at large mines than among miners at small mines (37.6% versus 11.7%; p<0.0001), and among miners at underground mines than among miners at surface mines (31.0% versus 18.9%; p<0.0001). Estimated participation rates for miners at mines at which at least one miner was examined were 34.4% for noncontract underground miners and 31.9% for surface miners. Reported by: MRL Pon, MPH, RA Roper, MS, Div of Health, Coal Mine Safety and Health, Mine Safety and Health Administration, US Dept of Labor. EL Petsonk, MD, ML Wang, MD, RM Castellan, MD, MD Attfield, PhD, GR Wagner, MD, Div of Respiratory Disease Studies, National Institute for Occupational Safety and Health, CDC. Editorial Note:To reduce the occurrence of occupational respiratory disability among coal miners, the Coal Mine Health and Safety Act of 1969 established limits on permissible dust exposures in underground coal mines and a radiographic screening program for underground coal miners. As mandated by the act, underground miners determined to have radiographic evidence of CWP are offered frequent exposure monitoring to ensure that their exposure to respirable dust is <1.0 mg/m3, and wage rates are retained if a job transfer is necessary to limit dust exposure. Miners with PMF are qualified to receive Federal Black Lung benefits. During 1970--1995, CWP prevalence declined markedly (4--6), highlighting an intended outcome of dust control in underground coal mines. The findings in this report indicate a continuing decline in CWP prevalence for underground miners with tenures of >20 years but no clear trend for those with tenures of <20 years (Figure 2). CWP continues to occur among working coal miners, even among those first employed after the current federal exposure limit became effective. The results raise concern about possible excessive exposures experienced by miners in several states, at smaller mines, and by some surface and contract miners. Both CWXSP and MCP address data quality and control biases by specifying standardized radiographic technique, by using only approved facilities and radiographic equipment, and by employing a standardized approach for assigning final determinations of radiograph classifications based on independent readings of each radiograph by multiple certified readers. The findings in this report are subject to at least four limitations. First, the programs are restricted to employed miners and are voluntary. Second, participation rates were low, especially among contract miners and miners at small mines. Third, work history data (e.g., tenure and date of first employment in mining) were not obtained consistently for all examinees. Finally, the effect of resulting potential participation biases on the generalizability of the aggregate results beyond the examinees is not clear, and the prevalences of CWP and PMF among all working or retired U.S. coal miners cannot be determined from available data. However, the general validity of these results is supported by the consistent relations observed over time between CWP prevalence and year of first employment, age, and tenure. Estimated participation rates were based on approximate denominators derived from the required quarterly reporting to MSHA of mine employment by coal operators. Several factors probably reduced participation rates: 1) MCP was not available at all surface mines; 2) at some underground mines, miners were not offered radiographs as required by CWXSP; and 3) not all of the underground miners included in denominators based on MSHA employment reports were employed during their mine's 6-month examination period. MCP was initiated in response to recommendations to enhance medical screening and health surveillance of coal miners (7) and has shown some early success in increasing participation of coal miners. The experience with this program is being reviewed to identify approaches that might result in sustained improvements in participation. Radiographic screening and surveillance programs protect the health of coal miners by detecting CWP and PMF in miners, allowing for preventive intervention focused on affected miners. Through aggregate analyses of screening results, these programs also can identify apparent high-risk subgroups that warrant further evaluation and appropriate intervention. However, primary prevention through general control of occupational exposure to coal mine dust remains essential for preventing CWP. To reduce the risk for lung disease among coal miners, MSHA has initiated rule-making efforts to ensure adherence to the current 2 mg/m3 or applicable respirable dust standard for underground coal mines during every work shift (8). NIOSH has recommended that MSHA lower the permissible exposure limit for respirable coal mine dust from 2 mg/m3 to 1 mg/m3 (9,10). References
* Persons who perform mining-related tasks, either underground or at the surface, for other business entities that coal mine owners or operators contract with for services.
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 4/17/2003 |
|||||||||
This page last reviewed 4/17/2003
|