|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
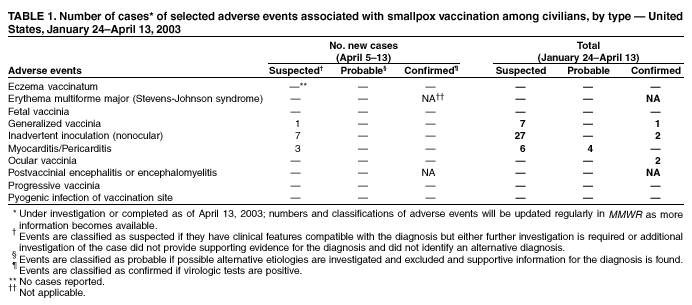
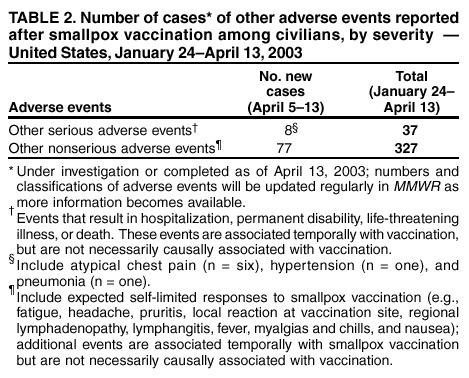
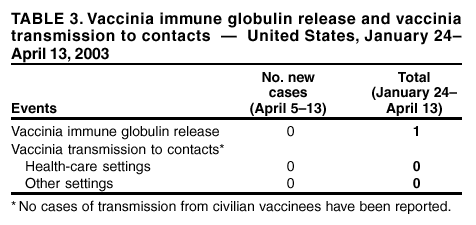
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Adverse Events Following Civilian Smallpox Vaccination --- United States, 2003During January 24--April 13, 2003, smallpox vaccine was administered to 32,644 civilian health-care and public health workers in 54 jurisdictions as part of an effort to prepare the United States for a possible terrorist attack using smallpox virus. This report updates information on all vaccine-associated adverse events among civilians vaccinated since the beginning of the vaccination program and among contacts of vaccinees, received by CDC from the Vaccine Adverse Event Reporting System (VAERS) as of April 13. In this vaccination program, CDC, the Food and Drug Administration, and state health departments are conducting surveillance for vaccine-associated adverse events among civilian vaccinees (1). As part of the vaccination program, civilian vaccinees receive follow-up care, and persons with reported adverse events after vaccination receive necessary medical attention. The U.S. Department of Defense is conducting surveillance for vaccine-associated adverse events among military vaccinees and providing follow-up care to those persons with reported adverse events. Adverse events that have been associated with smallpox vaccination are classified on the basis of evidence supporting the reported diagnoses. Cases verified by virologic testing are classified as confirmed. Cases are classified as probable if possible alternative etiologies are investigated and excluded and supportive information for the diagnosis is found. Cases are classified as suspected if they have clinical features compatible with the diagnosis, but either further investigation is required or investigation of the case did not provide supporting evidence for the diagnosis. All reports of events that follow vaccination are accepted (i.e., events associated temporally); however, reported adverse events are not necessarily associated causally with vaccination, and some or all of these events might be coincidental. As of April 13, a total of 10 cases of myopericarditis have been reported (Table 1); three are new reports received during April 5--13. During the same period, one new case of generalized vaccinia and seven new cases of inadvertent inoculation (nonocular) were reported. During the vaccination program, no cases of eczema vaccinatum, erythema multiforme major, fetal vaccinia, postvaccinial encephalitis or encephalomyelitis, progressive vaccinia, or pyogenic infection of the vaccination site have been reported (Table 1). During April 5--13, eight other serious adverse events were reported. Discharge diagnoses for these events were atypical chest pain (n = six), hypertension (n = one), and pneumonia (n = one) (Table 2). During April 5--13, a total of 77 other nonserious events were reported (Table 2). Among the 327 vaccinees with reported other nonserious adverse events during January 24--April 13 (Table 2), the most common signs and symptoms were fever (n = 68), rash (n = 59), headache (n = 49), pain (n = 49), and pruritus (n = 45). All of these commonly reported events are consistent with mild expected reactions following receipt of smallpox vaccine. Some vaccinees reported multiple signs and symptoms. During this reporting period, no vaccinia immune globulin was released for civilian vaccinees. No cases of vaccine transmission from civilian vaccinees to their contacts have been reported during the vaccination program (Table 3). Thirteen cases of transmission from military personnel to civilian contacts have been reported. Surveillance for adverse events during the civilian and military smallpox vaccination programs is ongoing; regular surveillance reports will be published in MMWR. Reference
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
Page converted: 4/17/2003
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 4/17/2003