|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
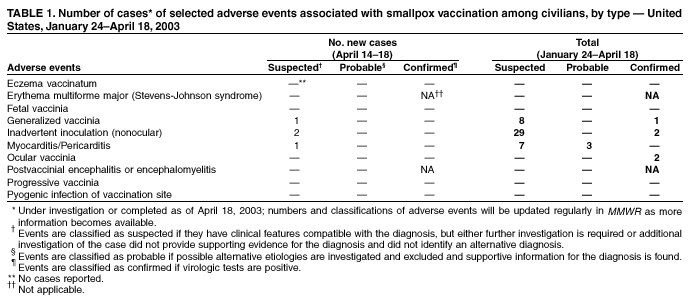
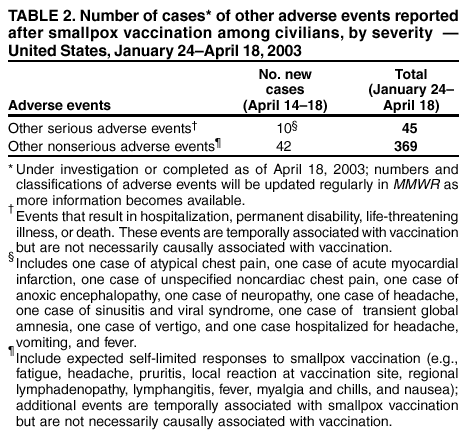
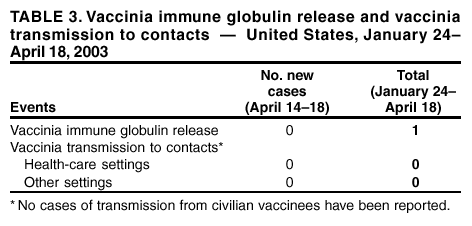
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Adverse Events Following Civilian Smallpox Vaccination --- United States, 2003During January 24--April 18, 2003, smallpox vaccine was administered to 33,444 civilian health-care and public health workers in 54 jurisdictions to prepare the United States for a possible terrorist attack using smallpox virus. This report updates information on vaccine-associated adverse events among civilians vaccinated since the beginning of the program and among contacts of vaccinees, received by CDC from the Vaccine Adverse Event Reporting System (VAERS) as of April 18. In this vaccination program, CDC, the Food and Drug Administration, and state health departments are conducting surveillance for vaccine-associated adverse events among civilian vaccinees (1). As part of the vaccination program, civilian vaccinees receive routine follow-up, and reported adverse events after vaccination receive follow-up as needed. The U.S. Department of Defense is conducting surveillance for vaccine-associated adverse events among military vaccinees and providing follow-up care to those persons with reported adverse events. Adverse events that have been associated with smallpox vaccination are classified on the basis of evidence supporting the reported diagnoses. Cases verified by virologic testing are classified as confirmed. Cases are classified as probable if possible alternative etiologies are investigated and excluded and supportive information for the diagnosis is found. Cases are classified as suspected if they have clinical features compatible with the diagnosis, but either further investigation is required or investigation of the case did not provide supporting evidence for the diagnosis. All reports of events that follow vaccination are accepted (i.e., events associated temporally); however, reported adverse events are not necessarily associated causally with vaccination, and some or all of these events might be coincidental. As of April 18, a total of 10 cases of myopericarditis have been reported (Table 1); one new report was received during April 14--18. During the same period, one new case of acute myocardial infarction (MI) was reported. Five cases of acute MI were previously reported (1,2) Case 1. A woman aged 56 years with no history of heart disease was revaccinated on April 1. Approximately 1 week later, she had palpitations and was noted to have premature ventricular contractions on cardiac monitor. She did not report chest pain. On April 15, cardiac consultation indicated an effusion on her echocardiogram and mitral regurgitation. A working diagnosis of myocarditis/pericarditis was made. The patient was treated with nonsteroidal anti-inflammatory drugs and investigation continues. Case 2. A man aged 49 years with no personal or family history of coronary artery disease was revaccinated on March 12. On the evening of April 7, he had an episode of chest pain that he attributed to indigestion. On April 8, while driving, he experienced increasingly severe chest pain, dyspnea, and diaphoresis. In the emergency department, an electrocardiogram showed nonspecific ST- and T-wave abnormalities and poor R-wave progression, all consistent with an anterior MI. Total creatine kinase and troponin-I assays were substantially elevated. Cardiac catheterization indicated an anterior MI caused by complete occlusion of the left anterior descending artery. Successful percutaneous transcoronary angioplasty and stent placement were performed, and the patient managed with aspirin, heparin, and intravenous beta-blockers. He is recovering at home. During April 14--18, one new case of generalized vaccinia and two cases of inadvertent inoculation (nonocular) were reported. During the vaccination program, no cases of eczema vaccinatum, erythema multiforme major, fetal vaccinia, postvaccinial encephalitis or encephalomyelitis, progressive vaccinia, or pyogenic infection of the vaccination site have been reported (Table 1). During April 14--18, in addition to the MI, nine other serious adverse events were reported, including one case of atypical chest pain and one case of anoxic encephalopathy (Table 2). Also during this period, 42 other nonserious events were reported (Table 2). Among the 369 vaccinees with reported other nonserious adverse events during January 24--April 18, the most common signs and symptoms were fever (n = 78), rash (n = 69), headache (n = 56), and pain (n = 56) (Table 2). All of these commonly reported events are consistent with mild expected reactions following receipt of smallpox vaccine. Some vaccinees reported multiple signs and symptoms. During the current reporting period, information was received about one inadvertent contamination of a vaccine vial when a vaccinator was observed placing a needle from a vaccinee back into the vial, then removing the needle from the vial and discarding it. The vial was then used to vaccinate additional persons, but new needles were used. The initial vaccinee was tested for hepatitis B virus, hepatitis C virus, and human immunodeficiency virus; all tests were negative. Investigation is ongoing for evidence of any complications from this event. During this reporting period, no vaccinia immune globulin was released for civilian vaccinees. No cases of vaccine transmission from civilian vaccinees to their contacts have been reported during the vaccination program (Table 3). A total of 14 cases of transmission from military personnel to civilian contacts have been reported. Surveillance for adverse events during the civilian and military smallpox vaccination programs is ongoing; regular surveillance reports will be published in MMWR. Reported by: Smallpox vaccine adverse events coordinators; National Immunization Program, CDC. Editorial Note:This report highlights the need to ensure proper infection-control procedures to avoid contamination of multidose vials. A recent supplement to the Advisory Committee on Immunization Practices (ACIP) recommendations for using smallpox vaccine states that the needle should not be reinserted into the vaccine vial (3). CDC's Smallpox Fact Sheet (http://www.bt.cdc.gov/agent/smallpox/vaccination/vaccination-method.asp) states that the same needle should never be dipped into the vaccine vial more than once to avoid contamination of the vaccine vial (4). Immediately after use, each presterilized needle should be disposed of in a biohazard waste container for sharp objects. Potentially contaminated vials should be discarded. Vaccinees who receive potentially contaminated vaccine should be offered follow-up testing for infectious diseases of concern, if possible, based on knowledge of test results from the initial vaccinee. Incidents of potentially inappropriate administration of smallpox vaccine should be reported to VAERS at http://www.vaers.org. This report includes cases reported as of April 18 that are either under investigation or have a reported final diagnosis. Because of ongoing discussions of final case definitions, numbers and classifications of adverse events might change and will be updated regularly in MMWR. References
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 4/24/2003 |
|||||||||
This page last reviewed 4/24/2003
|