Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Notice to Readers: Pneumococcal Conjugate Vaccine Shortage Resolved
In February 2000, Prevnar™, a 7-valent pneumococcal conjugate vaccine manufactured by Wyeth Lederle Vaccines (Pearl River, New York), was licensed for use among infants and young children. Beginning in August 2001, the supply of Prevnar™
failed to meet demand, resulting in shortages for health-care providers and health departments. To conserve the limited
supply and ensure protection of children at highest risk, CDC published interim recommendations for vaccination that called
for withholding vaccine from healthy children aged
>2 years and deferring some doses for healthy children aged <2 years
(1,2). Despite the shortage, introduction of the vaccine has been associated with a 69% decline in invasive disease among
children aged <2 years through 2001 (78% for vaccine serotypes and 50% for vaccine-related serotypes)
(3).
Vaccine production and deliveries are now adequate to permit a return to the routine vaccination schedule
(4). According to data from CDC tracking systems and the manufacturer, the average number of vaccine doses delivered monthly for each of the preceding 3 months exceeded the monthly estimated average national need, and all back orders have been filled in
both the public and private sectors.
According to the original Advisory Committee on Immunization Practices recommendations
(4) and more recent guidance from CDC
(5), all children aged <24 months and 24--59 months who are at increased risk for pneumococcal disease
(e.g., children with sickle cell disease or anatomic asplenia, chronic illness, a cerebrospinal fluid leak, a cochlear implant, or an immunocompromising condition) should be administered the pneumococcal conjugate vaccine. In addition, providers
should consider vaccine for all other children aged 24--59 months, with priority given to children aged 24--35 months, American Indian/Alaska Native and black children, and those who attend group child care.
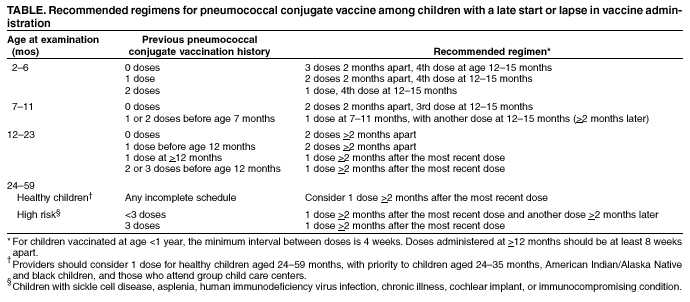
A catch-up schedule is provided for children who are incompletely vaccinated (Table). The highest priority for catch-up vaccination is to ensure that children aged <5 years at high risk for invasive pneumococcal disease because of
medical conditions have received a complete series. Second priorities include vaccination of healthy children aged <24 months who have not received any doses of pneumococcal conjugate vaccine and healthy children aged <12 months who have not
yet received 3 doses.
Because of the frequency of health-care provider visits for children during their first 18 months, catch-up
vaccination might occur at regularly scheduled visits for most children who receive vaccines from their primary-care provider; special notification should be considered for children who have completed their 15-month visit and are not scheduled to be
seen again before the visit at age 2 years. Programs that provide vaccinations but do not see children routinely for other reasons also should consider a notification process to contact undervaccinated or unvaccinated children.
Reporting Invasive Pneumococcal Disease Among Vaccinees
CDC is investigating situations in which invasive pneumococcal disease occurs despite vaccination. Health-care
providers are encouraged to report invasive pneumococcal disease occurring in children aged <5 years who have received >1 doses of pneumococcal conjugate vaccine to CDC through state health departments. If pneumococcal isolates are available from vaccinated children, CDC will perform serotyping to determine whether the strain is a type included in the
vaccine. Additional information is available at
http://www.cdc.gov/nip/diseases/pneumo/PCV-survrpts/default.htm.
CG Whitney, MM Farley, J Hadler, et al. Decline in invasive pneumococcal disease after the introduction of protein--polysaccharide
conjugate vaccine. N Engl J Med 2003;348:1737--46.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
[email protected].