|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
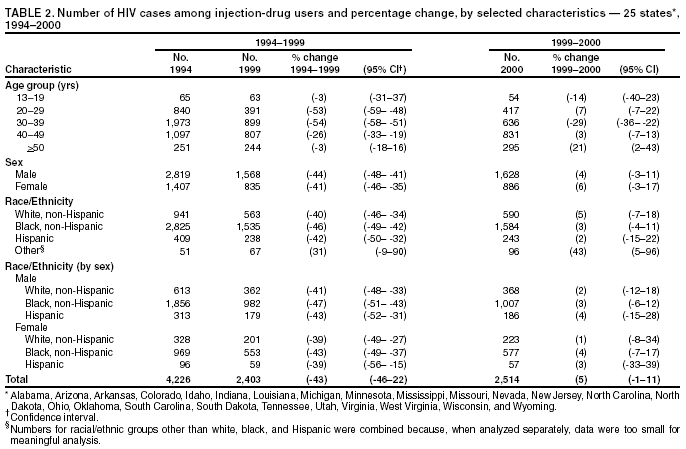
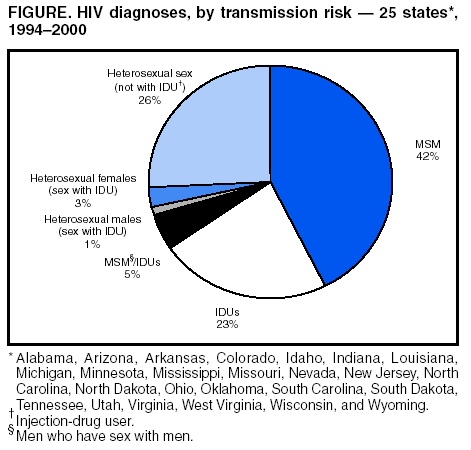
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. HIV Diagnoses Among Injection-Drug Users in States with HIV Surveillance --- 25 States, 1994--2000Injection-drug use is a risk factor for acquired immunodeficiency syndrome (AIDS) (1). Of the 765,559 cumulative AIDS cases diagnosed as of December 2000, a total of 193,527 (25%) occurred among injection-drug users (IDUs) (2). IDUs become infected with human immunodeficiency virus (HIV) through sharing injection-drug equipment with HIV-infected persons or by engaging in other risk behaviors such as having unprotected sex (3). Since 1995, AIDS incidence among IDUs has declined (2,4). This report presents data on initial HIV diagnoses among IDUs aged >13 years, with and without AIDS at the time of HIV diagnosis, by year, during 1994--2000. The findings indicate that HIV diagnoses among IDUs have leveled in the majority of demographic groups during this period in the 25 states for which HIV surveillance data are available*. Because IDUs and their sex partners represent approximately one third of persons infected in the HIV epidemic and continue to be at risk for transmitting HIV, prevention efforts targeting IDUs and their sex partners should be enhanced. Data were available from health departments in 25 states that have had HIV-infection case reporting since 1993, the first year for which HIV surveillance data were available. During 1993--2000, these states accounted for 516,939 (24%) AIDS case reports and 35,548 (7%) cases reported among IDUs. Data were adjusted for reporting delays. Cases reported without risk information were reclassified based on a probability formula (5). Annual proportions of HIV diagnoses among IDUs during 1994--2000 were compared by age, sex, and race/ethnicity, and 95% confidence intervals were computed for percentage differences. During 1994--2000, a total of 21,687 HIV diagnoses reported in the 25 states were among IDUs; males accounted for 14,252 (66%) cases. HIV diagnoses reported among IDUs declined 42% overall, compared with a 15% decrease among men who have sex with men (MSM) and a 9% increase among persons with heterosexual transmission during the same period. IDU-related HIV diagnoses declined from 4,226 cases in 1994 to 2,403 cases in 1999, and leveled to 2,514 from 1999 to 2000. Blacks continue to be represented disproportionately (65%) among IDU-related HIV cases diagnosed (Table 1). During 1994--2000, IDU-related HIV diagnoses declined among persons aged 13--19 years and 30--39 years by 17% and 68%, respectively. Among persons aged 20--29 years and 40--49 years, diagnoses decreased 53% and 26%, respectively, during 1994--1999, and leveled off during 1999--2000. IDU-related HIV diagnoses among persons aged >50 years were level during 1994--1999 and increased slightly during 1999--2000 (Table 2). Among men, HIV diagnoses reported among IDUs declined 44%, from 2,819 in 1994 to 1,568 in 1999, and leveled to 1,628 in 2000. Among women, diagnoses declined 41%, from 1,407 in 1994 to 835 in 1999, and leveled to 886 in 2000 (Figure). Trends were similar in all racial/ethnic groups. Among whites, IDU-related HIV diagnoses decreased 40%, from 941 in 1994 to 563 in 1999, and leveled to 590 in 2000. Among blacks, HIV diagnoses among IDUs decreased 46%, from 2,825 in 1994 to 1,535 in 1999, and leveled to 1,584 in 2000. Among Hispanics, IDU-related HIV diagnoses decreased 43%, from 409 in 1994 to 238 in 1999, and leveled to 243 in 2000 (Table 2). Asians/Pacific Islanders and American Indians/Alaska Natives accounted for 205 (1%) cases diagnosed during 1994--2000. Sex partners of IDUs accounted for 5,117 (4%) HIV infections diagnosed in these 25 states during 1994--2000 (Figure). Heterosexual men and women who reported having sex with IDUs accounted for 1,849 (1%) and 3,268 (3%) cases, respectively. MSM/IDUs accounted for 4,626 (5%) HIV diagnoses. All IDU-related HIV diagnoses, including those among IDUs, sex partners of IDUs, and MSM/IDUs, accounted for 31,428 (32%) diagnoses, compared with MSM (not IDUs) (39,184 [42%]) and those reporting having heterosexual sex (not with an IDU) (23,674 [25%]) (Figure). Reported by: LM Lee, PhD, M McKenna, MD, Div of HIV/AIDS Prevention, National Center for HIV, STD, and TB Prevention; TT Sharpe, PhD, EIS Officer, CDC. Editorial Note:The finding of overall declines in new HIV diagnoses among IDUs in the 25 states with HIV infection reporting is consistent with studies that suggest a decline in new HIV infections among IDUs in other areas of the United States (6). Several factors probably account for the decline. Because the peak of infections occurred in the early 1990s (2), the decline during the late 1990s might reflect the natural decline in the epidemiologic curve following the peak in the epidemic, which often is observed after the onset of a disease in a population. The decline also might be attributable in part to advances in antiretroviral therapy since 1995. In addition, the HIV epidemic among IDUs is closely related to other risk behaviors such as having unprotected sex, which frequently occurs in the context of illicit substance use (7). Changes in HIV prevalence among sex and needle-sharing partners or changes in risk behavior with such partners might lead to changes in the risk for new infections. The finding that IDU-related HIV diagnoses occurred disproportionately in males and blacks is consistent with the disproportionate impact of the HIV/AIDS epidemic on minority communities and the concentration of IDUs among males (2). The leveling of IDU-related HIV diagnoses during 1999--2000 for the majority of demographic groups might represent a plateau in IDU-related HIV diagnoses or changes in testing behavior among IDUs (6). In addition, the increase in IDU-related HIV diagnoses among persons aged >50 years during 1999--2000 might represent the aging of a cohort of IDUs who continue risk behaviors, acquire new infections, or receive late testing and diagnosis. IDUs who continue risk behaviors and sex partners of IDUs who contract the disease might represent missed opportunities for HIV prevention. Approximately 25% of the estimated 850,000--950,000 persons living in the United States with HIV are unaware of their infection (8), and some transmit HIV infections to others. In 2003, CDC launched a new strategy for prevention aimed at reducing the number of new infections in the United States by increasing the proportion of infected persons who know their status and by working with persons with HIV and their partners (9). The findings in this report are subject to at least three limitations. First, the data are from 25 states with <10% of IDUs with AIDS and are not generalizable to other states. Second, redistribution of risk is derived by using an algorithm based on historical patterns of risk determination after additional information is gathered; the summary might not account for current patterns of risk redistribution. Finally, the data include new HIV diagnoses, not new infections. Although testing patterns can change the number and trends of new diagnoses, surveillance methods being developed by CDC will enable estimation of patterns in HIV-infection incidence (10). CDC recommends that all states, especially those with high AIDS morbidity, implement HIV case surveillance. In addition, procedures to reassign cases reported without risk should be improved. CDC is piloting new methods to improve risk ascertainment, including statistical sampling and inference. Despite overall decreases, IDUs and their sex partners bear a substantial burden of the disease. Expansion of efforts that include counseling and voluntary HIV testing for IDUs and their sex partners is encouraged. Persons with HIV should receive counseling to reduce risks associated with transmission to others through drug use and sexual behaviors. Prevention programs targeting minority communities should continue. Drug treatment for IDUs, medical treatment for HIV-positive IDUs, and programs to prevent initiation of injection-drug use should be enhanced to prevent HIV infection and transmission among IDUs and their sex and drug-sharing partners. References
* Alabama, Arizona, Arkansas, Colorado, Idaho, Indiana, Louisiana, Michigan, Minnesota, Mississippi, Missouri, Nevada, New Jersey, North Carolina, North Dakota, Ohio, Oklahoma, South Carolina, South Dakota, Tennessee, Utah, Virginia, West Virginia, Wisconsin, and Wyoming.
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 7/10/2003 |
|||||||||
This page last reviewed 7/10/2003
|