|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
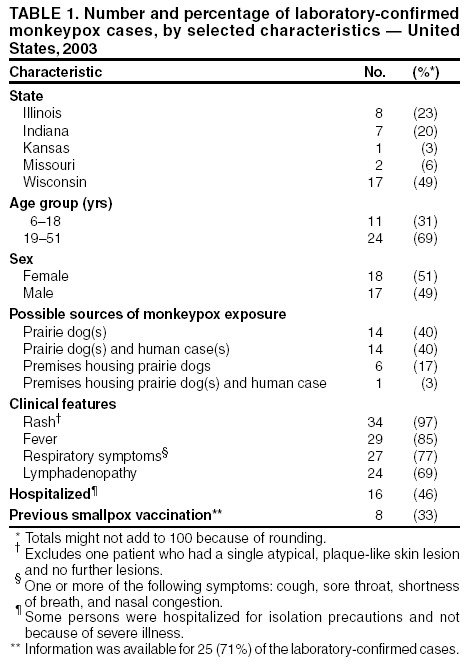
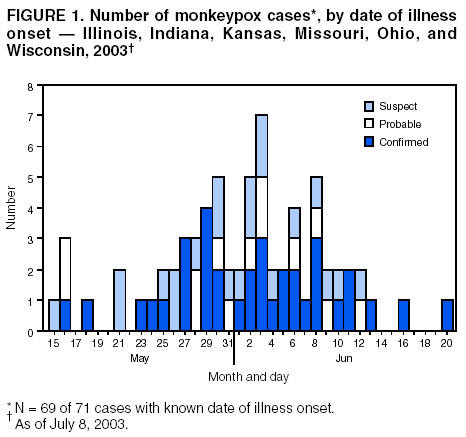
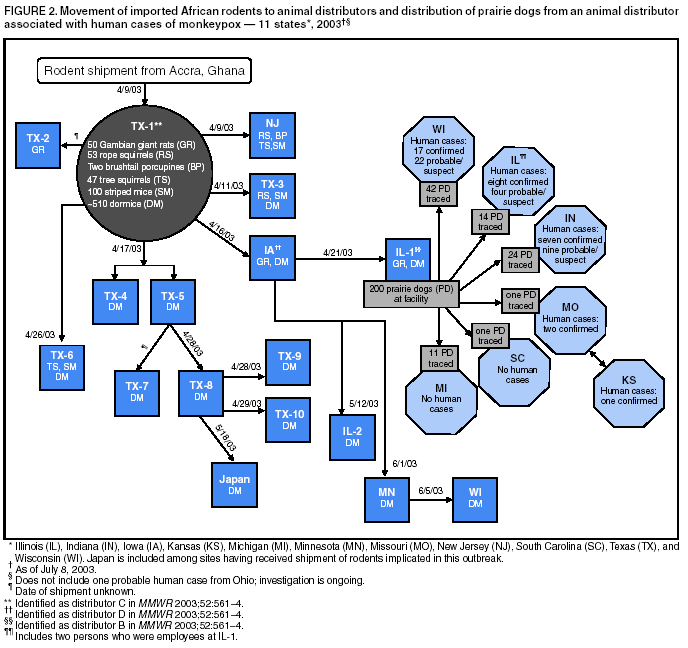
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Multistate Outbreak of Monkeypox --- Illinois, Indiana, Kansas, Missouri, Ohio, and Wisconsin, 2003CDC and state and local health departments continue to investigate cases of monkeypox among persons in the United States who had contact with wild or exotic mammalian pets or with persons with monkeypox (1--4). This report updates results of the epidemiologic investigation, provides information on the use of smallpox vaccine during the outbreak, and summarizes the animal tracing activities to identify the origin and subsequent distribution of infected animals. Epidemiologic InvestigationAs of July 8, 2003, a total of 71 cases of monkeypox have been reported to CDC from Wisconsin (39), Indiana (16), Illinois (12), Missouri (two), Kansas (one), and Ohio (one); these include 35 (49%) cases laboratory-confirmed at CDC and 36 (51%) suspect and probable cases under investigation by state and local health departments (Figure 1). Eleven cases were excluded from those reported previously because they met the exclusion criteria outlined in the updated national case definition, and one new case was added (1). The number of cases increased from May 15 through the week ending June 8 and declined subsequently; the date of onset for the last case was June 20. Of the 71 cases, 39 (55%) occurred among females; the median age was 28 years (range: 1--51 years). Age data were unavailable for one patient. Among 69 patients for whom data were available, 18 (26%) were hospitalized; some patients were hospitalized for isolation precautions only. Two patients, both children, had serious clinical illness (1--4); both of these patients have recovered. The majority of patients were exposed to prairie dogs. Some patients were exposed in premises where prairie dogs were kept, and others were exposed to persons with monkeypox. No patients have been confirmed to have had exposure to persons with monkeypox as their only possible exposure. Of the 35 laboratory-confirmed cases, 32 (91%) tested positive for monkeypox by polymerase chain reaction (PCR), culture, immunohistochemical testing (IHC), and/or electron microscopy in skin rash lesions; two tested positive by PCR and/or culture of an oropharyngeal or nasopharyngeal swab; and one tested positive by PCR and culture of a lymph node aspirate. For laboratory-confirmed cases, onset of illness ranged from May 16 to June 20. The majority of patients reported a clinical illness that included rash (one patient had a single, atypical plaque-like skin lesion) and fever (Table 1). The median incubation period* was 12 days (range: 1--31 days). Use of Smallpox VaccineTo prevent transmission of monkeypox, 30 persons (28 adults and two children) in six states have received smallpox vaccine since June 13. Vaccine was administered pre-exposure to seven persons (three veterinarians, two laboratory workers, and two health-care workers) and post-exposure to 23 persons (10 health-care workers, seven household contacts, three laboratory workers, one public health veterinarian, one public health epidemiologist, and one work contact). No serious adverse events were reported following smallpox vaccination, and no requests for vaccinia immune globulin have been received. Among the 30 persons who received smallpox vaccine, three (10%) reported rash within 2 weeks of vaccination. One of the three was confirmed as having monkeypox; another person had two skin lesion specimens that tested negative for orthopoxvirus and varicella zoster virus at the state health laboratory; no specimens were obtained for the third person who reported a single, dime-sized, pruritic and erythematous skin lesion (not pustular) remote from the vaccination site that appeared 4 days after vaccination and faded within a week. Animal Traceback and Trace-Forward InvestigationsTraceback investigations have determined that all 35 confirmed human cases of monkeypox were associated with prairie dogs obtained from an Illinois animal distributor (IL-1), or from animal distributors who purchased prairie dogs from IL-1 (Figure 2). Traceback of animal exposures are ongoing for other cases. Prairie dogs at IL-1 appear to have been infected through contact with Gambian giant rats and dormice that originated in Ghana and were purchased on April 21 by IL-1. Approximately 200 prairie dogs had been at the IL-1 facility during April--May; an unspecified number overlapped with the arrival of the imported African rodents on April 21 and probably were exposed to monkeypox. A total of 93 infected or potentially infected prairie dogs were traced from IL-1 to six states (Figure 2); in addition, an unknown number of prairie dogs died or were reportedly sold (as pets for sale or exchange) at animal swap meets for which no records were available for tracing. At CDC, laboratory testing of four prairie dogs originating from IL-1 confirmed the presence of monkeypox virus by PCR and IHC. Traceback investigations to identify the source of introduction of monkeypox into the United States identified a Texas animal distributor (TX-1) that had imported a shipment of approximately 800 small mammals from Ghana on April 9 that contained 762 African rodents, including rope squirrels (Funiscuirus sp.), tree squirrels (Heliosciurus sp.), Gambian giant rats (Cricetomys sp.), brushtail porcupines (Atherurus sp.), dormice (Graphiurus sp.), and striped mice (Hybomys sp.). CDC laboratory testing of some animals from this shipment confirmed the presence of monkeypox by PCR and virus isolation in several rodent species, including one Gambian rat, three dormice, and two rope squirrels (1). Trace-forward investigations of the rodents on the shipment were initiated before the availability of laboratory results because of concerns that animals were a potential source of continued spread of monkeypox (Table 2; Figure 2). Of the 762 rodents from the original shipment, 584 (77%) have been traced to distributors in six states. A total of 178 (23%) African rodents could not be traced beyond the point of entry in Texas because records were not available. No suspect, probable, or confirmed cases of human monkeypox have been associated with direct contact with the African rodents from the April 9 shipment. In addition, other than the prairie dogs traced from IL-1 to subsequent sites, no cases of monkeypox in other animals that had contact with the African rodents from the April 9 shipment have been reported. Reported by: State and local health departments. Monkeypox investigation team, CDC. Editorial Note:The outbreak described in this report highlights the public health threat posed by importation, for commercial purposes, of exotic pets into the United States. Epidemiologic and animal traceback investigations confirm that the first community-acquired human cases of monkeypox in the United States resulted from contact with infected prairie dogs that had been housed or transported with African rodents imported from Ghana. Imported, exotic wild animals can carry nonindigenous, zoonotic pathogens, which can spread rapidly among indigenous susceptible animal populations in the United States, particularly when mixed together in close proximity. In addition, interspecies exchange of pathogens is possible because of close relations between humans and their pets. In this outbreak, the rapid and widespread distribution of monkeypox-infected and potentially infected imported wild animals to distributors and potential buyers in several settings (e.g., pet stores, swap meets, and wild animal trade centers) in the United States and to other countries enabled epizootic spread through multiple states before effective interventions could be implemented. Public health strategies to control this outbreak, including the Food and Drug Administration-CDC joint order banning importation and prohibiting movement of the implicated animal species (http://www.cdc.gov/ncidod/monkeypox/pdf/embargo.pdf), state-enacted measures to further restrict intrastate animal shipment and trade (4), premise quarantine, and animal euthanasia, appear to have been effective in reducing exposure of humans to infected animals, with few cases reported since its implementation on June 11. Additional control measures have included pre- and post-exposure vaccination of potentially exposed persons with smallpox vaccine (5). Laboratory tests have demonstrated the presence of monkeypox virus in several rodents from the original shipment from Ghana that died unexpectedly and did not exhibit characteristic signs of monkeypox in animals (e.g., conjunctivitis, lymphadenopathy, and skin lesions). For this reason, CDC guidance for premise quarantine and animal euthanasia (http://www.cdc.gov/ncidod/monkeypox/quarantineremoval.htm) is based on the possibility that infected rodents from the April 9 shipment could be asymptomatic, shed virus, and potentially cause infection in other susceptible animals or humans. Although no human monkeypox cases have been associated with contact with rodents from the April 9 shipment, these animals are considered to pose a continued risk for infection for other animals and humans. Euthanasia, following American Veterinary Medical Association guidelines (http://www.avma.org/noah/members/policy/default.asp), is recommended for all rodents from the April 9 shipment and for any prairie dogs that were on the premises at the same time as any of the African rodents. In addition, mammals in facilities that housed a rodent from the April 9 shipment should be placed under quarantine for 6 weeks following the last date a rodent of concern was present. Efforts are underway to collect additional epidemiologic and laboratory data on both human and animal cases and their contacts, including animal handlers who might have been exposed to infected rodents. Importation of exotic animals and indigenous, wild animals harvested for the commercial pet trade have been associated with previous outbreaks of infectious diseases in humans, including salmonella associated with reptiles (e.g., lizards, snakes, and turtles) and tularemia associated with prairie dogs (6,7); prairie dogs also have been documented to be infected with other human pathogens (e.g., plague) (8). The Institute of Medicine recently highlighted the role of international travel and commerce in the emergence of infectious diseases through the dissemination of pathogens and their vectors throughout the world (9). CDC and other federal agencies, in collaboration with state and local health departments and professional organizations, are developing long-term strategies to coordinate the control of importation, exportation, interstate trade, and intrastate sale of exotic and native wild animals (10). Health-care providers, veterinarians, and public health officials who suspect monkeypox in animals or humans should report such cases to their state and local health departments. State health departments should report suspect cases to CDC, telephone 770-488-7100. An updated case definition with revised case exclusion criteria is available at http://www.cdc.gov/ncidod/monkeypox/index.htm. Rash illnesses suspected to be monkeypox should be confirmed by laboratory evaluation. Clinical specimens should be submitted for testing after consultation with the state and local health departments. Protocols for specimen collection, including completion of specimen submission forms, should follow CDC guidance available at http://www.cdc.gov/ncidod/monkeypox/diagspecimens.htm. Because information included in the specimen-submission and case-reporting forms is essential for accurate interpretation of laboratory results, these forms should be completed by state health departments. Preferred specimens for testing are those from skin lesions. Because smallpox vaccine might modify monkeypox disease, evaluation of any rash postvaccination in a person exposed to monkeypox should include laboratory testing for monkeypox virus. References
* Defined as first possible exposure date to illness onset date; however, some persons reported intermittent or continuous exposure.
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 7/10/2003 |
|||||||||
This page last reviewed 7/10/2003
|