|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
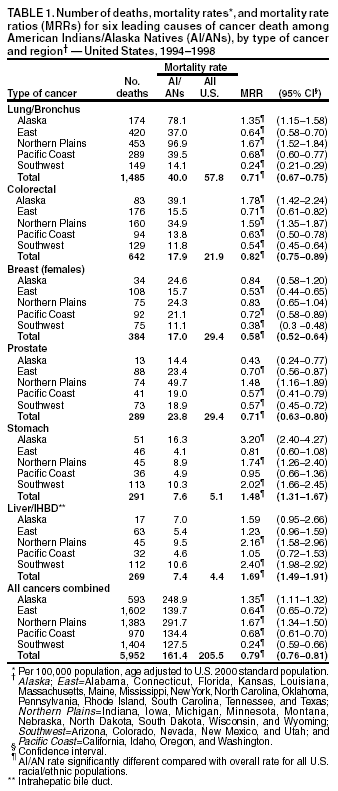
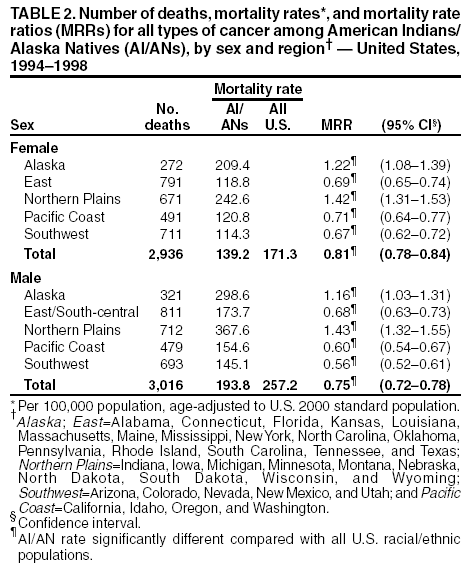
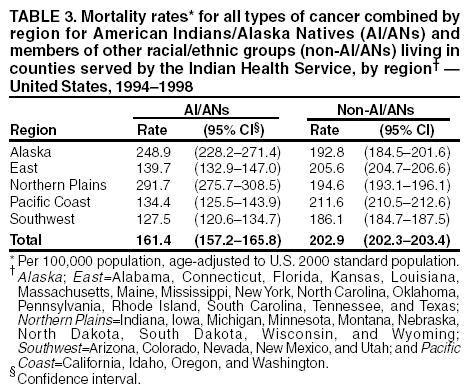
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Cancer Mortality Among American Indians and Alaska Natives --- United States, 1994--1998In the United States, public health interventions to control infectious diseases, lower infant and maternal mortality, and improve basic sanitation have led to a substantial increase in life expectancy for American Indians and Alaska Natives (AI/ANs). During 1940--1995, average life expectancy among AI/ANs increased 39%, from 51 years in 1940 to 71 years in 1995; however, AI/ANs experienced a parallel increase in mortality rates for chronic diseases, including cancer, which is the second leading cause of death for AI/ANs nationally and the leading cause of death among Alaska Natives (1,2). A previous study examining cancer mortality rates during 1989--1993 documented lower cancer mortality rates for AI/ANs than for the overall U.S. population, with regional variation (3). To understand cancer mortality among AI/ANs subsequent to that period, the Indian Health Service (IHS) and CDC analyzed death certificate data provided by CDC's National Center for Health Statistics for deaths among AI/ANs in five U.S. geographic regions* during 1994--1998. This report summarizes the results of that analysis, which indicate that cancer mortality rates among AI/ANs nationally were lower than cancer mortality rates for all U.S. racial/ethnic populations combined. Rates for AI/ANs varied by region, with the highest rates found in the Alaska and the Northern Plains regions. Plans or modifications for cancer prevention and treatment programs should account for regional variation, and programs to discourage smoking initiation, encourage tobacco cessation, and promote colorectal cancer screening among AI/ANs in the Alaska and the Northern Plains regions should be expanded. The analysis was limited to deaths of persons classified as AI/ANs on death certificates who at death were residents of counties on or adjacent to tribal reservations recognized by the Federal government (i.e., counties served by IHS). Denominator data for rate calculations for AI/ANs in the same counties reflected adjustments made to intercensal estimates for 1994--1998 on the basis of the 2000 decennial census (4). The AI/AN population of these counties comprised approximately 60% of persons in the United States who identified themselves as AI/ANs in the decennial census. Annualized mortality rates per 100,000 population adjusted to the 2000 standard population were calculated by using 10-year age intervals for the five regions. In addition, mortality rate ratios (MRRs) and 95% confidence intervals were calculated to compare rates with the overall U.S. population (5). The overall cancer mortality rate among AI/ANs (161.4 per 100,000 population) was lower than the U.S. rate for all racial/ethnic populations combined (205.5) (Table 1). The cancer mortality rate was 193.8 for males and 139.2 for females (Table 2). Rates were higher than the overall U.S. rate in the Alaska (248.9) and the Northern Plains regions (291.7); in both regions, excess mortality was attributed to cancer of the lung, colorectum, liver, stomach, and gallbladder. In contrast, the lung cancer mortality rate among AI/ANs in the Southwest region was fourfold lower than the overall U.S. rate for all racial/ethnic populations combined. Cervical cancer mortality rates were higher among AI/ANs than among all racial/ethnic populations (3.7 and 2.6, respectively), particularly in the East and Northern Plains regions, and breast cancer mortality rates were lower among AI/ANs than among all racial/ethnic populations (17.0 and 29.4, respectively), particularly in the East, Pacific Coast, and Southwest regions. Rates for lung cancer mortality, the leading cause of cancer death for all AI/AN populations combined, varied by region; rates in the Alaska (78.1) and the Northern Plains regions were higher than the U.S. rate for all racial/ethnic populations combined (57.8) but low in the Southwest region (14.1). Rates for colorectal cancer, the second most common cause of AI/AN cancer mortality, also varied by region. The Alaska and the Northern Plains regions had the highest MRRs (1.78 and 1.59, respectively), and the Southwest region (0.54) had the lowest; in other regions, MRRs were below the overall U.S. rates for all racial/ethnic populations combined. In the East region, 80% of AI/AN cancer deaths occurred among AI/ANs living in Oklahoma. Reported by: R Paisano, MHSA, N Cobb, MD, National Epidemiology Program, Indian Health Svc. DK Espey, MD, Div of Cancer Prevention and Control, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:Although the cancer mortality rate for AI/ANs was lower than the U.S. rate for all racial/ethnic populations combined, rates were higher for some cancer types and varied by region. In particular, mortality rates for all types of cancer combined were higher among AI/ANs in the Alaska and Northern Plains regions than the overall U.S. rate for all racial/ethnic populations combined. Rates for lung cancer mortality were consistent with known regional patterns of cigarette smoking for AI/AN communities across the United States (6). Although colorectal cancer mortality patterns are more difficult to account for than regional variation in lung cancer mortality, contributing factors might include diet, physical activity levels, genetic predisposition, and access to, or use of, clinical preventive services. Although breast cancer mortality rates were lower among AI/AN women in all regions than among all U.S. women, breast cancer is the second leading cause of cancer death among AI/AN women. Few breast cancer screening services were available to AI/AN women before the National Breast and Cervical Cancer Early Detection Program (NBCCEDP) was established in 1990. From its inception, this program has emphasized breast cancer screening services for AI/AN women and provided screening mammograms to approximately 58,000 AI/AN women, in whom 610 breast cancers have been detected (NBCCEDP, personal communication, 2003). In the majority of regions, prostate cancer mortality rates were lower among AI/ANs than among all racial/ethnic populations combined. However, the rate among Northern Plains AI/AN men was nearly 50% higher than the rate for all racial/ethnic populations combined. In contrast, stomach and liver/intrahepatic bile duct (IHBD) cancer mortality rates for AI/ANs were generally higher than overall U.S. rates. Helicobacter pylori infection in stomach cancer and the synergistic effect of alcohol abuse and chronic infection with hepatitis B and C in liver/IHBD cancer might contribute to these disparities (7). The findings in this report are subject to at least four limitations. First, because the racial identities of some cancer decedents probably were coded incorrectly (8), cancer mortality rates in AI/AN populations probably are underestimated. Second, some rates are based on small numbers of cases and have corresponding wider confidence intervals; these should be interpreted with caution. Third, causes of death for AI/ANs are more likely to be misclassified as "symptoms, signs, and ill-defined conditions" than they are for whites (9). In addition, the results might be confounded by residence because the majority of the study population reside in rural areas. However, rates for non-AI/ANs calculated for the IHS service counties and for the same geographic regions were similar to U.S. rates for all racial/ethnic populations combined (Table 3). Finally, racial misclassification for AI/ANs varies by region (10). The extent of this variability within IHS service counties is not known. Plans or modifications for cancer prevention and treatment programs should account for regional variation, and programs to discourage smoking initiation, encourage tobacco cessation, and promote colorectal cancer screening among AI/ANs in the Alaska and Northern Plains regions should be expanded. In addition, efforts are needed to improve the accuracy of vital records data collection by reducing misclassification of racial/ethnic groups; projects are underway at the state and national levels to match key state vital records databases and the National Death Index with the IHS patient registration database so persons who have been misclassified can be identified correctly. References
* Alaska; East=Alabama, Connecticut, Florida, Kansas, Louisiana, Maine, Massachusetts, Mississippi, New York, North Carolina,Oklahoma, Pennsylvania, Rhode Island, South Carolina, Tennessee, and Texas; Northern Plains=Indiana, Iowa, Michigan, Minnesota, Montana, Nebraska, North Dakota, South Dakota, Wisconsin, and Wyoming; Southwest=Arizona, Colorado, Nevada, New Mexico, and Utah; and Pacific Coast=California, Idaho, Oregon, and Washington.
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 7/31/2003 |
|||||||||
This page last reviewed 7/31/2003
|