|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
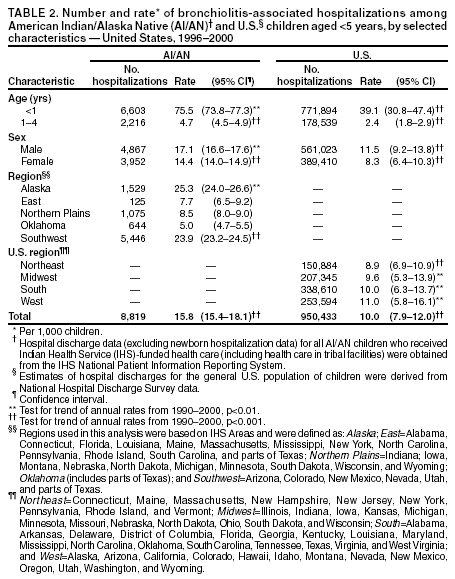
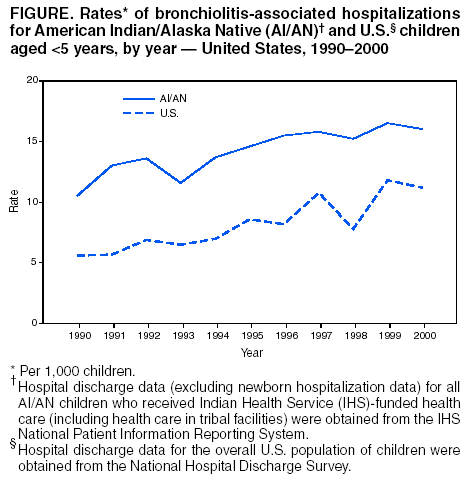
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Bronchiolitis-Associated Outpatient Visits and Hospitalizations Among American Indian and Alaska Native Children --- United States, 1990--2000Respiratory syncytial virus (RSV) is the most common cause of lower respiratory tract infection (LRTI) in young children worldwide. Approximately half of all LRTI-associated hospitalizations are caused by bronchiolitis, with RSV accounting for 50%--80% of all bronchiolitis cases (1). Bronchiolitis is an infection of the bronchial and bronchiolar epithelial cells, with subsequent inflammation and edema resulting in airway obstruction. This process manifests clinically as cough, wheezing, tachypnea, and respiratory distress. Because of the association between bronchiolitis and RSV infection, bronchiolitis is a good indicator of RSV disease; therefore, prevention strategies for RSV should reduce the rate of bronchiolitis. Rates of bronchiolitis-associated hospitalization for American Indian/Alaska Native (AI/AN) children are approximately twice that for the general population of U.S. children (2,3). This report describes the first estimate of rates of outpatient bronchiolitis-associated visits and updates rates of bronchiolitis-associated hospitalizations in these populations. Rates of bronchiolitis-associated outpatient visits and hospitalizations were higher for AI/AN children than for other U.S. children, and hospitalization rates for both groups increased during 1990--2000. This report underscores the high burden of bronchiolitis and the need for effective prevention programs for AI/AN communities. Outpatient visits and hospitalizations associated with the diagnosis of bronchiolitis (International Classification of Diseases, 9th revision, Clinical Modification, code 466.1) were analyzed for children aged <5 years. Outpatient visit data (including clinic and emergency department visits) for 1999--2000 were obtained from the Indian Health Service (IHS) National Patient Information Reporting System (NPIRS) for all AI/AN children who received IHS-funded health care (including health care in tribal facilities) (4) and from the National Ambulatory Medical Care Survey (NAMCS) and National Hospital Ambulatory Medical Care Survey (NHAMCS) for children in the overall U.S. population (5). Hospital discharge data (excluding newborn hospitalization data) for 1990--2000 with bronchiolitis listed as a diagnosis were obtained from IHS (6) and the National Hospital Discharge Survey (NHDS) (7). The Direct and Contract Health Service Inpatient IHS Dataset comprises all AI/AN patient discharge records obtained from IHS- and tribally operated hospitals and from hospitals that have contracted with IHS or tribes to provide health-care services to federally recognized AI/AN tribes within the United States. The IHS California and Portland, Oregon, administrative areas were excluded from the hospitalization data analysis because neither had any IHS- or tribally operated hospitals. NHDS is a representative sample of discharge records from short-stay, nonfederal general and children's hospitals in the United States. NAMCS, NHAMCS, and NHDS do not include data on outpatient visits or hospitalizations from within the IHS/tribal system (5,7). For this report, the units of analysis were hospitalizations and outpatient visits. Rates of outpatient visits for 1999--2000 and hospitalizations for 1996--2000 were calculated as the number of visits or hospitalizations per 1,000 children. AI/AN population denominators were determined for each year of the study by using the IHS 2002 user population estimates and adjusting retrospectively for annual changes in the IHS service population (using February 2002 IHS area estimates) (8). The user population included all registered AI/ANs who received IHS-funded health care at least once during the preceding 3 years. In this study, AI/AN children aged <5 years represented those who received health care through IHS- or tribally operated facilities. U.S. outpatient visit and hospitalization rates were calculated by using the U.S. resident population census and natality data as the denominators (9,10). Annual and overall standard errors of NAMCS/NHAMCS and NHDS estimates were calculated by using SUDAAN to account for the stratified sampling techniques (5,7). Tests for trend during 1990--2000 for annual hospitalization rates were performed for AI/AN hospitalization rates by using linear regression, and weighted least squares regression was used for U.S. hospitalization rates. Outpatient VisitsDuring 1999--2000, the average annual rate for bronchiolitis-associated outpatient visits among AI/AN children aged <5 years was 108.8 per 1,000 children, which was significantly higher than the rate for children aged <5 years in the overall U.S. population (42.2) (Table 1). Outpatient visit rates for AI/AN children were more than three times greater than the rate for U.S. children, among both infants (aged <1 year) (452.3 versus 146.2, respectively) and children aged 1--4 years (46.5 versus 13.7, respectively). The rate among AI/AN boys (119.5) was higher than the rate for girls (97.7), and both were more than twice the rates among U.S. children overall (41.2 and 43.3, respectively). Among AI/AN children, rates varied by region*, with the highest rates found in the Alaska (162.4) and Southwest (164.7) regions. HospitalizationsDuring 1996--2000, AI/AN children aged <5 years had average annual rates of bronchiolitis-associated hospitalizations that were approximately twofold higher than the overall rate for U.S. children, among both infants (75.5 versus 39.1, respectively) and children aged 1--4 years (4.7 versus 2.4, respectively) (Table 2). Among AI/AN children, the Alaska (25.3) and Southwest (23.9) regions had high hospitalization rates, and the other three regions had low rates that were similar to the overall rate for U.S. children. The hospitalization rates for the Alaska and Southwest regions increased significantly during 1990--2000, as did the overall rate for U.S. children (p<0.005) (Figure). During the study period, the median length of stay for AI/AN and U.S. children overall was 3 days per hospitalization (interquartile range: 2--4 days). A total of 36 (0.41%) hospital deaths were reported at discharge among AI/AN children. Reported by: K Carver, PhD, Office of Program Support; JE Cheek, MD, Epidemiology Program, Indian Health Svc. RC Holman, MS, AT Curns, MPH, JS Bresee, MD, JR Lingappa, MD, LJ Anderson, MD, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; AJ Peck, MD, EIS Officer, CDC. Editorial Note:The findings in this report indicate that rates of both bronchiolitis-associated outpatient visits and hospitalizations were higher for AI/AN children than for the overall population of U.S. children. These findings are consistent with bronchiolitis-associated hospitalization rates reported previously, with the highest rates in the youngest age group and in the Alaska and Southwest regions (1--3). In addition, hospitalization rates increased for AI/AN children living in these regions and for the overall population of U.S. children. Possible risk factors associated with higher rates of bronchiolitis in AI/AN children include household crowding and underventilation, smoke exposure, and lack of breast-feeding. Methodologic factors, including differences in health-care use, patient management by different health-care systems, and illness coding and data reporting by different groups, also might have contributed to the disparity between AI/AN children and the overall population of U.S. children and among regions. Similarly, the cause of increasing bronchiolitis-associated hospitalization might be related to several factors, including changing criteria for hospital admission as a result of the use of pulse oximetry and improved survival of high-risk premature infants, resulting in a larger population of premature infants susceptible to severe RSV disease (1). The findings in this report are subject to at least two limitations. First, AI/AN children described in this study received IHS-funded health care and might not be representative of all AI/AN children in the United States. Second, AI/ANs eligible for IHS/tribal services could have received medical care outside of the IHS/tribal system, which would result in an underestimate of outpatient and hospitalization rates among AI/ANs. However, AI/ANs probably seek IHS/tribal medical care because it is provided without cost. This study highlights a disproportionate burden of bronchiolitis in AI/AN children relative to the overall population of U.S. children and the need and opportunity to identify strategies to improve health in this population. Because RSV is the most common etiology for bronchiolitis, strategies to prevent RSV probably would decrease the burden of bronchiolitis substantially. However, the only available effective preventive therapies for RSV, intravenous RSV immune globulin and intramuscularly administered monoclonal antibody (palivizumab), are indicated for a small percentage of children (i.e., high-risk, premature infants) and are not expected to affect overall hospitalization rates. A safe and efficacious RSV vaccine would provide the best opportunity to prevent a substantial percentage of bronchiolitis disease. Continued efforts are needed to identify and better understand host factors and environmental risk factors for bronchiolitis for targeted preventive strategies (e.g., campaigns to decrease parent smoking) to have a more immediate impact on decreasing disease burden among children, especially those in AI/AN communities. Acknowledgments This report is based on contributions by P Smith, N Cobb, Y Cadman, L Petrakos, L Querec, S Kaufman, Indian Health Svc. M Owings, Div of Health Care Statistics, National Center for Health Statistics; R Singleton, MD, Alaska Native Tribal Health Consortium and Arctic Investigations Program; D Ingram, Div of Health and Utilization Analysis, National Center for Health Statistics; C Chesley, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases, CDC. References
* Regions used in this analysis were based on Indian Health Service Areas and were defined as: Alaska; East=Alabama, Connecticut, Florida, Louisiana, Maine, Massachusetts, Mississippi, New York, North Carolina, Pennsylvania, Rhode Island, South Carolina, and parts of Texas; Northern Plains=Indiana; Iowa, Montana, Nebraska, North Dakota, Michigan, Minnesota, South Dakota, Wisconsin, and Wyoming; Oklahoma (includes parts of Texas); and Southwest=Arizona, Colorado, New Mexico, Nevada, Utah, and parts of Texas.
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 7/31/2003 |
|||||||||
This page last reviewed 7/31/2003
|