|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
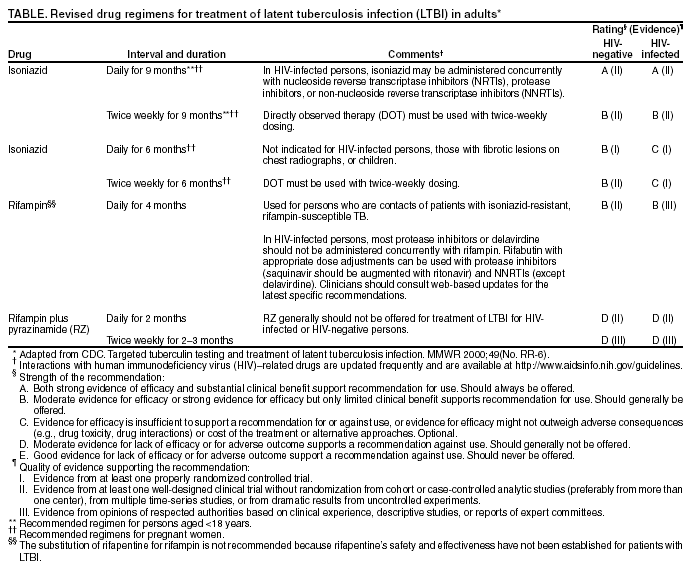
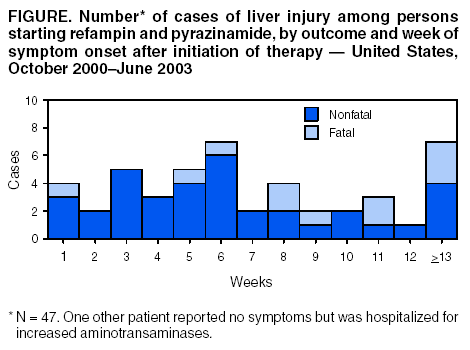
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Adverse Event Data and Revised American Thoracic Society/CDC Recommendations Against the Use of Rifampin and Pyrazinamide for Treatment of Latent Tuberculosis Infection---United States, 2003CDC has reported previously surveillance data of severe liver injury in patients treated for latent tuberculosis infection (LTBI) with a daily and twice-weekly 2-month* regimen of rifampin with pyrazinamide (RZ). On the basis of these initial reports, CDC cautioned clinicians in the use of this therapy with advised additional monitoring (1--4). To estimate the incidence of RZ-associated severe liver injury and provide more precise data to guide treatment for LTBI, CDC collected data from cohorts of patients in the United States who received RZ for the treatment of LTBI during January 2000--June 2002 and for whom data were reported to CDC through June 6, 2003. This report summarizes the analysis, which found high rates of hospitalization and death from liver injury associated with the use of RZ. On the basis of these findings, the American Thoracic Society (ATS) and CDC now recommend that this regimen should generally not be offered to persons with LTBI. The revised ATS/CDC recommendations described in this report have been endorsed by the Infectious Diseases Society of America (IDSA). Clinicians are advised to use the recommended alternative regimens for the treatment of LTBI (Table). Rifampin and pyrazinamide (PZA) should continue to be administered in multidrug regimens for the treatment of persons with active tuberculosis (TB) disease (5). For surveillance purposes, a case of severe liver injury was defined as one leading to the hospitalization or death of a patient being treated for LTBI with RZ (2). During October 2000--June 2003, CDC received reports of 48 patients who had confirmed cases; 33 (69%) cases occurred in the second month of treatment. A total of 11 (23%) patients died†, including two persons known to be infected with human immunodeficiency virus (HIV). A two-phase retrospective survey was conducted to estimate the incidence of severe liver injury among persons receiving RZ for treatment of LTBI. In December 2001 (phase I), CDC sent a questionnaire by e-mail to TB-control programs in 12 large cities and all 50 states, asking them to identify programs and health-care providers prescribing RZ for treatment of LTBI. All controllers responded, and in February 2002, CDC staff called the programs and health-care providers identified as prescribing RZ for LTBI to confirm its use. In September 2002 (phase II), CDC mailed a second questionnaire to the 150 health-care providers identified during the first phase, requesting aggregate cohort data for January 2000--June 2002; 109 (78%) health-care providers responded by June 6, 2003. Of 7,737 patients who were reported to have started RZ for treatment of LTBI during the survey period, 5,980 (77%) received daily doses, and 1,757 (23%) received twice-weekly doses. A total of 204 patients discontinued using RZ because of aspartate aminotransferase (AST) concentrations greater than five times the upper limit of normal (rate: 26.4 per 1,000 treatment initiations; 95% confidence interval (CI) = 22.8--30.0). An additional 146 patients discontinued using RZ because of symptoms of hepatitis (rate: 18.9 per 1,000 treatment initiations; 95% CI = 17.4--20.4). Of the 48 cases of severe liver injury reported to CDC through passive surveillance, 30 also were detected in the second phase of the survey. Of the 18 patients whose cases were not detected, six patients had liver injuries outside the survey period, five patients' health-care providers did not respond to the questionnaire, and seven (six of whom were in private practice) were not identified in the first phase of the survey. Of the 30 patients whose cases were detected, 23 (77%) recovered, and seven (23%) died. On the basis of these 30 cases, the estimated rates of hospitalization and death during the survey period were 3.0 (95% CI = 1.8--4.2) and 0.9 (95% CI = 0.2--1.6) per 1,000 treatment initiations, respectively. Reported by: State and territorial health depts. Div of Tuberculosis Elimination, National Center for HIV, STD, and TB Prevention, CDC. Editorial Note:The CDC cohort analysis found that the rates of severe liver injury and death related to the use of RZ are higher than the rates for isoniazid (INH)-associated liver injury in the treatment of LTBI. Although initial studies attributed hospitalization rates as high as 5.0 per 1,000 treatment initiations and mortality rates as high as 1.0 per 1,000 to INH (6,7), studies conducted since 1991 involving more than one million persons treated with INH have reported hospitalization rates of 0.1--0.2 (median: 0.15) and mortality rates of 0--0.3 per 1,000 (median: 0.04) (4,8,9). This decrease from earlier studies might reflect careful selection of patients and active monitoring for early signs of adverse events. In addition to the survey on the use of RZ described in this report, recent studies have reported episodes of liver injury and hospitalization associated with RZ for treatment of LTBI (10,11), including the need for transplantation in one patient (12). Among first-line agents in the treatment of active TB disease, pyrazinamide (PZA) might be the most hepatotoxic (13). These data and other recent studies (4,10,11,14--16) were reviewed by TB experts§ at a meeting held during the 99th International ATS Conference in Seattle, Washington, on May 12, 2003, to discuss proposed revisions to guidelines for the treatment of LTBI. ATS and CDC now recommend that this regimen should generally not be offered to persons with LTBI for either HIV-negative or HIV-infected persons. On the basis of the investigation of potential cofactors in the 48 patients with serious liver injury, this regimen should never be offered to patients who 1) are concurrently taking other medications associated with liver injury; 2) drink excessive amounts of alcohol, even if alcohol use is discontinued during treatment; 3) have underlying liver disease; or 4) have a history of INH-associated liver injury. If the potential benefits of this regimen outweigh the risk for severe liver injury and death associated with it, use of RZ might be considered in carefully selected patients, but only if 1) the preferred or alternative regimens (i.e., 9 months of daily or biweekly INH, 6 months of daily or biweekly INH, or 4 months of daily rifampin) are judged not likely to be completed and 2) oversight by a clinician with expertise in the treatment of LTBI can be provided. A TB/LTBI expert should be consulted before RZ is offered. In addition, patients should be asked whether they have had liver disease or adverse effects from taking INH or other drugs, informed of potential hepatotoxicity of the RZ regimen, and advised against the concurrent use of potentially hepatotoxic drugs, including over-the-counter drugs such as acetaminophen. To facilitate periodic clinical assessments of persons taking an RZ regimen (2), clinicians should dispense no more than a 2-week supply (with a daily PZA dose of <20.0 mg/kg/d [maximum daily PZA dose: 2.0 g], and a twice-weekly dose of <50.0 mg/kg/d [maximum twice-weekly PZA dose: 4.0 g]). Patients should be reassessed in person by a health-care provider at 2, 4, 6, and 8 weeks of treatment for adherence, tolerance, and adverse effects. The 8-week assessment also should be used to document treatment completion. At each visit, health-care providers who speak the patient's own language should instruct the patient to stop taking RZ immediately and seek medical consultation if abdominal pain, emesis, jaundice, or other symptoms of hepatitis develop. Provider continuity is recommended for optimal monitoring. For persons taking this regimen, serum aminotransaminases (AT) and bilirubin should be measured at baseline and at 2, 4, 6, and 8¶ weeks of treatment. Because the majority of these patients had onset of symptoms of liver injury after the fourth week of therapy (Figure), patients should be monitored throughout the entire course of treatment. Use of RZ should be discontinued immediately and not resumed for any of the following findings: 1) AT greater than five times the upper limit of normal range in an asymptomatic person, 2) AT greater than normal range when accompanied by symptoms of hepatitis, or 3) a serum bilirubin concentration greater than the normal range, whether or not symptoms are present. The risk for progression from LTBI to active TB is increased substantially in persons with HIV infection (4). Therefore, as recommended previously for the treatment of all persons in whom LTBI is diagnosed, voluntary HIV counseling and testing should be offered routinely. For progression to TB disease to be prevented, persons with LTBI should be identified in contact investigations and targeted screening programs and should complete treatment with safe and effective regimens. The successful treatment of LTBI is an essential component of the TB elimination strategy in the United States (4). In addition to this report, CDC and its partners are sending a letter to TB-control programs in 12 large cities and all 50 states and organizations active in TB control (e.g., the National Coalition to Eliminate Tuberculosis). To reach clinicians who are treating patients with LTBI, primary care medical associations (e.g., the American Medical Association and the American College of Physicians) are distributing this report to their members. This report and the letter are available at http://www.cdc.gov/tb. The letter is being added to the April 2000 CDC Targeted Tuberculin Testing and Treatment of Latent TB Infection Guidelines, and existing provider educational materials are being revised. The recommendations against the use of RZ for treatment of LTBI described in this report do not apply to the appropriate use of rifampin and PZA in multidrug regimens for the treatment of persons with active TB disease. In these circumstances, the risk for morbidity and mortality from TB disease is substantially greater than with LTBI. Rifampin and PZA are essential components of recommended ATS/CDC/IDSA regimens that render patients noninfectious rapidly and are effective in curing patients with drug-susceptible M. tuberculosis strains within 6 months (5). CDC continues to collect reports of severe liver injury leading to hospital admission or death in persons receiving any treatment for LTBI. Health-care providers are encouraged to report such events to CDC's Division of Tuberculosis Elimination, telephone 404-639-8442. Details of the RZ survey analysis and the case series will be described in a separate publication. References
* The twice-weekly rifampin and pyrazinamide regimen for treatment of LTBI was specified to be completed within 2--3 months. † Of the 11 deaths, eight were reported previously (1--3). § Representatives from state and local TB-control programs and health departments and hospitals, National TB Centers, ATS, the National Coalition to Eliminate Tuberculosis, the National Tuberculosis Controllers Association, Infectious Diseases Society of America, the American College of Chest Physicians, and CDC. CDC met separately with the Food and Drug Administration. ¶ In the interim revised recommendations, biochemical monitoring at 2, 4, and 6 weeks was recommended (2); however, because of the occurrence of serious adverse events late in the course of RZ treatment, monitoring at 8 weeks has been added.
Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 8/7/2003 |
|||||||||
This page last reviewed 8/7/2003
|