 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Methicillin-Resistant Staphylococcus aureus Infections Among Competitive Sports Participants --- Colorado, Indiana, Pennsylvania, and Los Angeles County, 2000--2003Although outbreaks of methicillin-resistant Staphylococcus aureus (MRSA) usually have been associated with health-care institutions, MRSA is emerging as a cause of skin infections in the community. This report summarizes several reported clusters of skin and soft tissue infections associated with MRSA among participants in competitive sports and identifies possible risk factors for infection (e.g., physical contact, skin damage, and sharing of equipment or clothing). The findings underscore 1) the potential for MRSA infections among sports participants; 2) the need for health-care providers to be aware that skin and soft tissue infections occurring in these settings might be caused by MRSA; and 3) the importance of implementing prevention measures by players, coaches, parents, and school and team administrators. FencersIn February 2003, the Colorado Department of Public Health and Environment was notified by a local health department about a cluster of MRSA infections among members of a Colorado fencing club and their household contacts. After club leaders reported five cases of infection to the local health department, all members (n = 70) of the fencing club were asked to complete a questionnaire that included questions about infections and possible risk behaviors such as sharing of clothing or equipment. A total of 62 (89%) fencers responded to the survey. No additional cases were identified from the survey. A confirmed case of MRSA infection was defined as signs and symptoms of an infection (e.g., fever, pus, swelling, or pain) during July 2002--February 2003 in a fencer or household contact of a fencer from whom MRSA was cultured from a clinical isolate. A probable case was defined as skin or soft tissue infection during the outbreak period in a fencer or household contact of a fencer from whom no clinical culture was obtained. Three confirmed and two probable cases were identified; one patient was a household contact. Median age of patients was 31 years (range: 11--51 years); three (60%) were female. One patient had paraspinal myositis with bacteremia and was hospitalized for 11 days. The other four patients reported one to six abscesses each, located on the legs or thighs (n = four), abdomen (n = three), axilla (n = one), buttocks (n = one), hand (n = one), and behind the knee (n = one). Three (60%) patients were hospitalized and received intravenous antimicrobial therapy. Two of the patients with confirmed cases reported recurrent infections for which they received antimicrobial therapy and made multiple health-care visits before their wounds were cultured. All patients have recovered. Pulsed-field gel electrophoresis (PFGE) testing was performed on isolates from two patients; an isolate from one of the patients with a confirmed case was not available. The PFGE patterns from both were indistinguishable. Facilities at the fencing club included changing rooms and practice areas. No showers were available. Although none of the fencers with infections reported sharing clothing, masks, and weapons, such sharing was common among team members. In addition, fencers wear a sensor wire under their clothes to record when they have been touched by an opponent's weapon. Interviews with club members indicated that these wires were shared routinely and had no routine schedule for cleaning. No other common sources of exposure outside of the fencing club were identified. Club members, coaches, and administrators were instructed in MRSA transmission control measures. These included 1) increased hand hygiene, 2) showering with soap after every practice or tournament, 3) covering cuts and abrasions with a bandage until healed, 4) laundering personal items such as towels and supporters after each use, 5) cleaning or laundering shared athletic equipment such as pads or helmets at least once a week but ideally after each use, 6) establishing a routine cleaning schedule for the sensor wires, and 7) consulting a health-care provider for wounds that do not heal or appear infected. No further infections have been reported. Football Players and WrestlersClusters of MRSA infection among sports team participants were identified during September 2000 in Pennsylvania and during the fall and winter of 2002--2003 in Indiana and Los Angeles County, California. Affected persons included college and high school--aged football players and wrestlers; the numbers of infected members per team ranged from two to 10 players. During September--October 2000, CDC assisted the Pennsylvania Department of Health in an investigation of an outbreak of MRSA culture-positive skin and soft tissue infections among 10 members of a Pennsylvania college football team, seven (70%) of whom were hospitalized. All isolates from the Pennsylvania athletes had indistinguishable PFGE patterns. Several possible risk factors for infection were identified, including skin trauma from turf burns and shaving and sharing of unwashed bath towels. In September 2002, the Los Angeles County Department of Health Services investigated two cases of MRSA skin infection among members of a college football team. Both patients were hospitalized; one received surgical debridement and skin grafts. Isolates from the two players had indistinguishable PFGE patterns. Team players reported frequent skin trauma and reported covering wounds approximately half of the time. In addition, health department staff identified the potential for spread through shared items such as balms and lubricants. In January 2003, the Indiana Department of Health was notified of two wrestlers on a high school team who had MRSA skin infections diagnosed. Neither patient was hospitalized, and isolates were not available for PFGE testing. The two players were in different weight groups and had never wrestled each other, suggesting that transmission could have occurred through sharing items rather than direct contact. No other common exposures were identified. Reported by: N Gantz, MD, Hospital A; H Harmon, MPH, J Handy, County A Health Dept, Colorado; K Gershman, MD, Colorado Dept of Public Health and Environment. J Butwin, MSN, Indiana State Dept of Health. L Mascola, MD, Los Angeles County Dept of Health Svcs, Los Angeles County, California. A Weltman, MD, R Groner, Pennsylvania Dept of Health. Div of Applied Public Health Training, Epidemiology Program Office; Div of Healthcare Quality Promotion, National Center for Infectious Diseases; A Cronquist, M Kainer, N Lee, EIS officers, CDC. Editorial Note:Outbreaks of community-associated MRSA (CA-MRSA) occur in various populations, including children attending child care, prison inmates, and men who have sex with men (1--3). This report demonstrates that CA-MRSA has the potential to spread and cause outbreaks among players of competitive sports, including those sports that involve little skin-to-skin contact among players, such as fencing. Physicians should be aware of the potential for MRSA infections in sports participants when evaluating patients and making treatment decisions. As demonstrated by this cluster of MRSA infections among fencers, patients with recurrent MRSA infections might make multiple health-care visits before a wound culture is obtained. Recurrence of infections might be avoided if physicians obtain cultures more routinely when athletes have infected wounds. Transmission of S. aureus, for both susceptible and antimicrobial resistant strains, usually occurs through close contact with a person who has either a draining lesion or asymptomatic carriage of S. aureus. Although the investigations described in this report did not determine the roots of MRSA transmission definitively, three factors might have contributed to transmission in these outbreaks. First, competitive sports participants might develop abrasions and other skin trauma, which could facilitate entry of pathogens. Even in sports with less direct contact, protective clothing can be hot and might chafe skin, resulting in abrasions and lacerations. Fencers reported developing skin rashes frequently under protective clothing. Second, some sports for which MRSA infections have been reported involve frequent physical contact among players (e.g., football and wrestling). S. aureus and other skin flora can be transmitted easily from person to person with direct contact. Third, sports such as fencing have limited skin-to-skin contact but require multiple pieces of protective clothing and equipment, which often might be shared. The use of shared equipment or other personal items that are not cleaned or laundered between users could be a vehicle for S. aureus transmission. Previous outbreaks of staphylococcal skin infection have been reported among wrestlers and rugby and football players (4--7). In these outbreaks, risk factors have included skin trauma (4,7) and contact with lesions of other players (7). The findings in this report, particularly the cluster of MRSA infections among participants in a sport with little skin-to-skin contact, suggest that sharing equipment or personal items also might facilitate MRSA transmission. Although none of the fencers reported sharing equipment or clothing items, their use of shared sensor wires was not assessed specifically. Maintaining good hygiene and avoiding contact with drainage from skin lesions of other players are the best methods for preventing spread of staphylococcal skin infections. Guidelines for preventing skin infections among sports team participants should be followed (6--10). All persons associated with competitive sports teams, including players, coaches, teachers, parents, and administrators, can help prevent sports-related skin infections and should be aware of prevention measures (Box). Sports team administrators should be encouraged to provide facilities and equipment necessary to promote good hygiene, such as clean facilities and adequate supplies of soap and towels. Coaches and parents should encourage good hygiene among players, and they should be taught to administer proper first aid, practice appropriate hand hygiene, and implement a system to ensure adequate wound care and to cover skin lesions appropriately before play. Players should be encouraged to practice good hygiene, avoid sharing towels or other personal items, and inform coaches about active skin infections. Additional information about MRSA is available at http://www.cdc.gov/ncidod/hip/aresist/mrsa.htm, or by telephone, 800-893-0485. References
Box 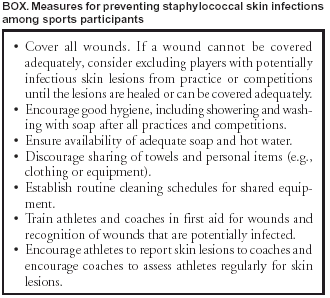 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 8/21/2003 |
|||||||||
This page last reviewed 8/21/2003
|