 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Injuries Associated with Landmines and Unexploded Ordnance --- Afghanistan, 1997--2002Landmines and unexploded ordnance (UXO) pose a substantial public health risk (1,2). Approximately 60--70 million landmines are scattered in approximately 70 countries (3), and an estimated 24,000 persons, mostly civilians, are killed or injured annually by landmines and UXO (4). In Afghanistan, approximately 5--7 million landmines are scattered throughout the country (4). During 2000--2001, Afghanistan had the highest number of reported landmine and UXO casualties in the world (5). This report presents analyses of surveillance data on landmine- and UXO-related injuries in Afghanistan during January 1997--September 2002, which indicate that the proportion of victims injured by UXO increased during this time, compared with the proportion injured by landmines. The majority (61%) of adult victims were injured by landmines, and the majority (66%) of children and adolescents were injured by UXO. Mine-risk education programs should focus on UXO hazards for children and on landmine hazards for adults and should address age-specific risk behaviors. Data on landmine- and UXO-related injuries were obtained from the United Nations Mine Action Center for Afghanistan (UN MACA), which conducts surveillance for these injuries in Afghanistan. The data include geographic location of incident, victim demographics, type of injury, type of explosive involved, activity at the time of injury, and other information about the circumstances of the incident. Approximately 70% of records in the database came from the clinic-based surveillance system operated by the International Committee of the Red Cross (ICRC), which uses both active and passive data-collection methods. ICRC clinic-based surveillance began in 1998 and has expanded during the observation period to include approximately 390 health clinics and hospitals in Afghanistan (6). The remaining data on landmine- and UXO-related injuries were collected from mine-clearance teams and community mine-risk education programs operated by the nongovernment organizations working in mine clearance, mine-risk education, and victim assistance under the auspices of UN MACA. Rates were not calculated because no reliable data were available on large population changes during 1997--2002 and the sensitivity of the system is unknown. Duplicate entries were excluded, and statistical analyses were performed by using JMP (version 5.0) software from SAS Institute. Statistical significance of associations was tested by using chi-square tests. During January 1997--September 2002, a total of 6,114 injuries from landmines and UXO were reported to UN MACA in Afghanistan. The number of reported victims of landmines and UXO was highest in 1999 and decreased gradually; sex and age distributions of victims remained relatively stable (Table 1). Injuries in males were approximately 10 times higher than in females. In each year during 1997--2002, approximately half of all injuries occurred in persons aged <18 years. The greatest number (1,830 [29%]) of injuries occurred in children aged 10--14 years, followed by persons aged 15--19 years (891 [14%]) and children aged 5--9 years (834 [13%]). During this period, the proportion of UXO-related injuries increased, and that of landmine-related injuries decreased (chi square for linear trend = 114.8; p<0.001). The proportion of children injured by UXO was 2.3 times as high as that of adults (chi square = 729.7; p<0.001) (Table 2). The proportion of adult victims sustaining amputation was 1.3 times higher than that of child victims (chi square = 67.7; p<0.001). The case-fatality rate was the same (approximately 7%) in both age groups. Children were injured most often while playing or tending animals; adults were injured most often while traveling or engaging in military activities (Table 2). Reported by: M Wennerstrom, United Nations Mine Action Center for Afghanistan, Kabul; S Baaser, P Salama, MD, United Nations Children's Fund, Kabul, Afghanistan. M Brennan, MD, BA Woodruff, MD, National Center for Environmental Health; O Bilukha, MD, EIS Officer, CDC. Editorial Note:The data presented in this report demonstrate that injuries from landmines and UXO remain a public health concern in Afghanistan. The majority of landmines were laid during the Soviet occupation in the 1980s (3); however, many areas have been newly contaminated with UXO during recent episodes of fighting between Taliban and allied forces (5). Mines often are laid around objects of economic importance (e.g., industrial buildings, roads, water sources, and fertile land), resulting in injuries among persons who are traveling or performing activities of economic necessity (e.g., farming, collecting wood or water, and tending animals). UXO often lie on the surface of the ground and thus are more visible and easier to avoid. However, because of their visibility, UXO pose a particular threat to children and adolescents who like to play or tamper with strange objects. The findings in this report are subject to at least four limitations. First, because surveillance for landmine- and UXO-related injuries is predominantly clinic-based, it probably undercounts victims who die before reaching the clinic, whose injuries are too minor to seek medical care, or who do not have access to medical facilities. The overall sensitivity of the system is unknown but is thought to be <50% (5,7). Second, the reported case-fatality rate probably is underestimated because surveillance detects predominantly victims who survive long enough to receive medical care. Survey data from Afghanistan and other countries have shown case-fatality rates as high as 50%--55% (8,9). Third, the time trends in recorded injuries should be interpreted with caution because of the low sensitivity of the system and variability in system coverage over time depending on the availability of resources, the security situation, and other factors. However, sensitivity of the system to landmine-related injuries versus sensitivity to UXO-related injuries probably has not changed substantially over time, suggesting that the data reflect a true increase in the proportion of UXO-related injuries among all recorded injuries. Finally, although this surveillance system identifies acute injuries, it does not monitor long-term disability or psychological impact on victims and their families, which can add substantially to the public health burden. The more restricted mobility of Afghan women and the resulting lower likelihood that women engage in activities that put them at risk for landmine- and UXO-related injuries might account for the low proportion of female victims. In addition, because of cultural restrictions, women, if injured, might be less likely to receive medical care or to be interviewed and recorded by the surveillance system. Among children aged <5 years, sex-specific differences in mobility generally do not apply, and the proportion of female victims is 35%. The increasing proportion of injuries from UXO and the high proportion of such injuries among children and adolescents underscore the need for effective mine-risk education programs for children and adolescents that focus on UXO hazards and address age-specific risk behaviors, such as playing, tending animals, and tampering with explosives. Mine-risk education programs for adults should focus more on hazards from landmines. Such programs also should address the approximately two million refugees who returned to Afghanistan in 2002 and who might be at higher risk for landmine- and UXO-related injuries because they are unaware of dangerous areas. Surveillance data about the incidence and types of injury sustained by victims of landmines and UXO should be instrumental in planning and implementing victim-assistance programs. Similarly, mine-clearance programs should use surveillance data to prioritize areas for clearance. Expansion of community-based reporting will improve sensitivity and representativeness of surveillance. Acknowledgment This report is based on data provided by the United Nations Mine Action Center for Afghanistan and the International Committee of the Red Cross. References
Table 1 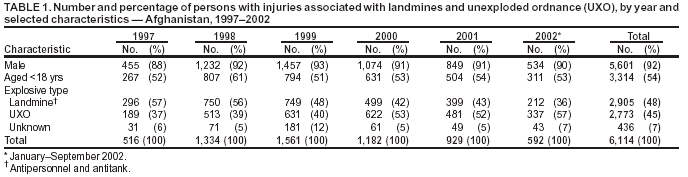 Return to top. Table 2 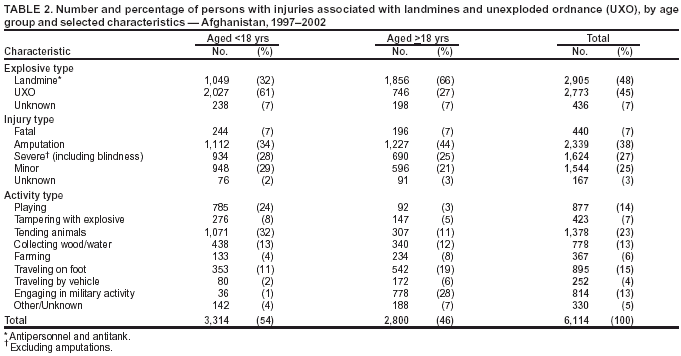 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 9/11/2003 |
|||||||||
This page last reviewed 9/11/2003
|