|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
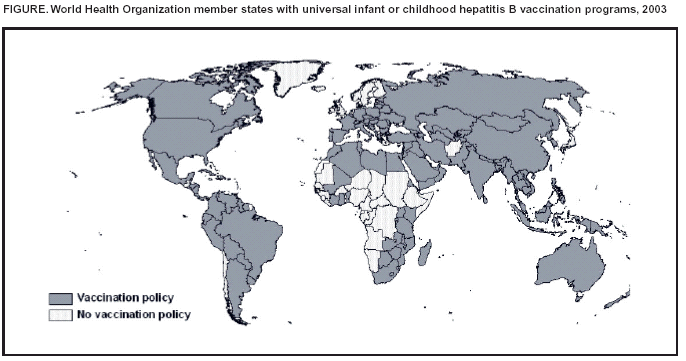
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Global Progress Toward Universal Childhood Hepatitis B Vaccination, 2003In 1992, the World Health Organization (WHO) set a goal for all countries to integrate hepatitis B vaccination into their universal childhood vaccination programs by 1997. This report summarizes the global progress achieved toward vaccination of children against hepatitis B virus (HBV) infection. Although many countries have introduced hepatitis B vaccination into their national vaccination programs, efforts are needed to increase coverage with the 3-dose hepatitis B vaccination series and expand vaccination programs into countries where the vaccine has not yet been introduced. In 2001, the most recent year for which complete program data are available, 126 (66%) of 191 WHO member states had universal infant or childhood hepatitis B vaccination programs (1). Through these programs, an estimated 32% of children aged <1 year were vaccinated fully with the 3-dose hepatitis B vaccination series. In the six WHO regions, the proportion of children aged <1 year who were vaccinated fully was 65% in the Western Pacific Region, 58% in the Americas Region, 45% in the European Region, 41% in the Eastern Mediterranean Region, 9% in the South-East Asian Region, and 6% in the African Region. As of May 2003, a total of 151 (79%) of 192* WHO member states had adopted universal childhood hepatitis B vaccination policies, including six that have policies for vaccinating adolescents (Figure). Of the 137 member states that have adopted universal childhood hepatitis B vaccination and for which data are available, 76 (55%) have a policy for administering the first dose of vaccine soon after birth (birth dose). Of the 89 member states with historically high prevalences of chronic HBV infection (i.e., prevalence of hepatitis B surface antigen [HBsAg] >8%) and for which universal infant hepatitis B vaccination is recommended specifically, 64 (72%) have adopted universal infant hepatitis B vaccination. Of these 64 member states, 34 (53%) have a policy for administration of a birth dose of vaccine. Goals for global hepatitis B vaccination are for the vaccine to be introduced in all countries by 2007 and for coverage with the 3-dose hepatitis B vaccination series to reach 90% by 2010 (2). Reported by: M Gacic-Dobo, G Mayers, M Birmingham, DVM, Dept of Vaccines and Biologicals, World Health Organization, Geneva, Switzerland. M Kane, MD, Children's Vaccine Program, Program for Appropriate Technology in Health, Seattle, Washington. SC Hadler, MD, Global Immunization Div, National Immunization Program; MJ Perilla, MPH, FE Shaw, MD, ST Goldstein, MD, EE Mast, MD, HS Margolis, MD, Div of Viral Hepatitis, National Center for Infectious Diseases; T Samandari, MD, EIS Officer, CDC. Editorial Note:Each year, approximately 600,000 HBV-related deaths occur worldwide (CDC and WHO, unpublished data, 2003). An estimated 93% of these deaths result from the chronic sequelae of HBV infection: cirrhosis and hepatocellular carcinoma (HCC) (CDC, unpublished data, 2003). Approximately 21% of HBV-related deaths result from infection acquired in the perinatal period and 48% from infection acquired in early childhood (age <5 years) (CDC, unpublished data, 2003). Therefore, vaccination of infants and children is the highest priority for hepatitis B vaccination programs. Three doses of hepatitis B vaccine are 90%--95% efficacious in preventing HBV infection and its chronic sequelae (3). To prevent perinatal HBV transmission, the first dose of vaccine should be administered within the first 24 hours after birth (3,4). Hepatitis B vaccination has been shown to reduce the prevalence of chronic HBV infection and the incidence of HCC dramatically. In The Gambia, the prevalence of chronic infection among children declined from 10.0% to 0.6% after implementation of universal infant hepatitis B vaccination (5). Similar declines in prevalence of chronic infection associated with infant and childhood hepatitis B vaccination have been demonstrated in China, Indonesia, Senegal, and Thailand, and among Alaska Natives (6,7). After implementation of universal infant hepatitis B vaccination in Taiwan, the incidence of HCC among children declined from 0.7 to 0.36 per 100,000 (8). Several important challenges remain to achieve the goal of global childhood hepatitis B vaccination introduction. Countries that have not yet introduced hepatitis B vaccine should do so. For many of these countries, this will require strengthening their existing vaccination program infrastructure to accommodate the addition of a new vaccine (9). In countries where the vaccine has been introduced already, coverage with the 3-dose hepatitis B vaccination series should be increased to that of the 3-dose diphtheria-tetanus-pertussis (DTP) series, and then to >90%. Countries that do not have a policy for administration of a birth dose of vaccine should consider the feasibility of implementing such a policy. In countries with high hepatitis B vaccination coverage among children, consideration should be given to catch-up vaccination of older children, adolescents, and adult populations at increased risk for HBV infection. A major barrier to the introduction of hepatitis B vaccination has been the high cost of hepatitis B vaccines. Although the price of monovalent hepatitis B vaccine for developing countries has decreased from approximately U.S.$3.00 per dose in 1990 to U.S.$0.30 per dose in 2001, the cost remains higher than that of the older vaccines (e.g., DTP, oral polio, and measles), which cost U.S.$0.06--$0.10 per dose. Since 1999, support from the Global Alliance for Vaccines and Immunization (GAVI) and the Vaccine Fund (VF) has accelerated introduction of hepatitis B vaccine in the world's poorest countries (9). As of May 2003, of 75 countries eligible for GAVI/VF support, 48 (64%) had received funding for hepatitis B vaccination introduction. Administration of a birth dose of vaccine presents a challenge. Worldwide, approximately 50% of infants are born at home and do not have immediate access to health care. However, because hepatitis B vaccine has been shown to be heat stable, it could be administered by trained birth attendants to infants born at home. The feasibility of such a strategy has been demonstrated in Indonesia, where trained birth attendants were taught to administer the birth dose of vaccine to infants born at home by using a single-use, pre-filled injection device (10). WHO, in collaboration with CDC and other GAVI partners, conducted process evaluations of hepatitis B vaccination introduction in five African countries where the vaccine had been introduced recently. These evaluations demonstrated that hepatitis B vaccine introduction did not negatively impact the existing vaccination programs, including coverage with the other childhood vaccines. However, several problems were identified related to the management of this relatively costly vaccine: vaccine freezing during storage and shipment, and vaccine wastage. Outcome evaluations are needed to document the impact of vaccination on the prevalence of chronic HBV infection and HBV-related morbidity and mortality. References
* In September 2002, Timor Leste (East Timor) became a WHO member state.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 9/11/2003 |
|||||||||
This page last reviewed 9/11/2003
|