|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
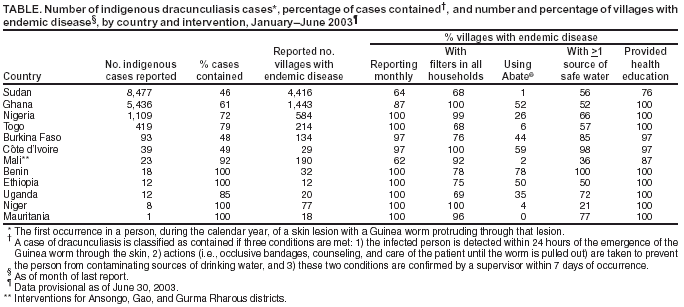
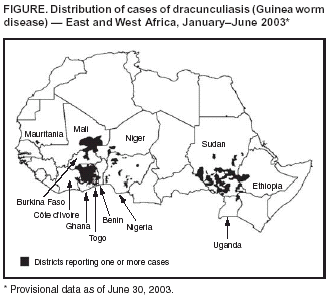
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Global Eradication of Dracunculiasis, January--June 2003In 1986, when the World Health Assembly adopted a resolution calling for the eradication of dracunculiasis (Guinea worm disease), an estimated 3.5 million persons in 20 countries had the disease, and approximately 120 million persons were at risk for infection (1,2). By the end of 2002, annual incidence of the disease had been reduced >98%; seven countries in which dracunculiasis formerly was endemic (Cameroon, Chad, India, Kenya, Pakistan, Senegal, and Yemen) were free of the disease, and four countries (Central African Republic, Ethiopia, Mauritania, and Uganda) reported <100 cases each. During 1993--2002, the number of villages outside Sudan that reported cases decreased from approximately 23,000 to 2,022. This report describes the status of the global Dracunculiasis Eradication Program (DEP)* as of June 2003. The data indicate that incidence of the disease outside Ghana and Sudan has declined substantially since June 2002. Continuing efforts in all countries in which the disease is endemic, intensified efforts in Ghana, and an end to the ongoing war in Sudan are required for the eradication of dracunculiasis. To conduct surveillance, village--based health-care workers (usually volunteers) search for infected persons (those with skin lesions and emerging Guinea worms) in each village with endemic disease and complete a register that serves as a basis for monthly zonal, district-, regional-, and national-level reports. In 2002, a total of 54,648 cases were reported in 6,255 villages in 12 African countries (3); 4,233 (68%) of those villages were in Sudan, which reported 41,493 (76%) cases. Outside Sudan, 573 villages reported five or more cases each. The World Health Organization (WHO) is investigating whether dracunculiasis is endemic in Central African Republic, which reported no cases in 2002 or during January--June 2003 (3) but which during previous years had reported cases imported from other countries and presumed indigenous cases. During January--June 2003, a total of 15,688 cases were reported in 12 African countries (Figure), including 8,477 (54%) from Sudan and 5,436 (35% ) from Ghana (Table), compared with 23,116 total cases reported during January--June 2002, including 16,871 (73%) from Sudan and 3,115 (13%) from Ghana. In West Africa, the disease is most endemic in Ghana, which had 75% of cases reported outside Sudan. During January--June 2003, Ghana reported 5,436 cases, 75% more than during the same period in 2002; 5,242 (96%) of these cases occurred in 15 (14%) of 110 districts. This increase reflects improved surveillance in these mostly contiguous northern districts. In mid-2002, with the help of increased technical assistance, Ghana enhanced its surveillance, investigations, and interventions. Since then, approximately 6,000 more village-based personnel have been mobilized, and all interventions have been improved in the 15 districts in which the disease burden is greatest. During January--June 2003, among 10 other countries with endemic disease, the number of reported cases declined 45%, compared with a reduction of 35% during the same reporting period in 2002 (4); the number of cases declined 44% in Nigeria, the country with the third-highest number of cases, and 60% in Benin, 63% in Burkina Faso, and 76% in Côte d'Ivoire. A total of 42 cases were exported from one country to another, including 18 from Sudan, 14 from Ghana, four from Togo, four from Niger, and one each from Mali and Nigeria. Nomadic Tuareg populations in the shared border areas of Burkina Faso, Mali, and Niger have endemic dracunculiasis infection and pose special challenges to programs in those countries. During January--June 2003, these three countries intensified interventions (e.g., distribution of more cloth filters and more extensive health education in communities in which the disease is endemic) and increased their coordination. In Togo, which reported 20% fewer cases during January--June 2003 than during the same period in 2002, the number of cases in two northern regions adjacent to areas of northern Ghana in which disease is highly endemic increased 100% (from 88 cases to 176). Togo is intensifying interventions in these regions, including voluntary isolation of patients in health-care facilities during their illness. Sudan's DEP is intervening in approximately 6,000 villages, primarily in the southern part of the country, where the civil war has prevented access to many areas in which disease is endemic. During January--June 2003, the eight affected northern states reported one indigenous case and five imported cases from southern Sudan, compared with three indigenous and nine imported cases during the same period in 2002. In the 3,613 villages in which Sudan's DEP intervened in 2001 and to which it still had access in 2002, dracunculiasis incidence declined 53% (from 45,761 cases to 21,321); however, newly accessed villages accounted for 49% of the cases reported in 2002. In anticipation of persons who were displaced internally returning to their homes after a peace agreement, Sudan's DEP has educated approximately 210,000 (34%) of the estimated 700,000 Sudanese in camps inside the country, and DEPs in Ethiopia, Kenya, and Uganda are doing the same for Sudanese refugees in camps there. Reported by: The Carter Center, Atlanta, Georgia. World Health Organization Collaborating Center for Research, Training, and Eradication of Dracunculiasis, Div of Parasitic Diseases, National Center for Infectious Diseases, CDC. Editorial Note:Dracunculiasis is a parasitic infection caused by Dracunculus medinensis. Persons become infected by drinking water from ponds contaminated by copepods (water fleas) that contain immature forms of the parasite; 1 year after entering the infected person, adult worms approximately 1 meter (40 inches) in length emerge through skin lesions, usually on the lower limbs, which frequently develop severe secondary bacterial infections. No effective treatment or vaccine for the disease exists, and infected persons do not become immune to future infections by the parasite. However, dracunculiasis can be prevented by 1) filtering drinking water through a finely woven cloth, 2) treating contaminated water with the larvicide Abate® (temephos), 3) educating persons to avoid entering water sources when Guinea worms are emerging from their bodies, and 4) providing clean water from bore-hole or hand-dug wells (5). DEPs continue to make progress toward dracunculiasis eradication in all countries with endemic disease other than Sudan and Ghana. In 2003, for the first time, Benin, Côte d'Ivoire, and Niger appear likely to report <100 indigenous cases. Benin (with 18 indigenous cases), Côte d'Ivoire (39 cases), Mauritania (one case), and Uganda (12 cases) appear close to interrupting transmission of the disease. However, armed conflict is delaying eradication in Côte d'Ivoire, Ethiopia, and Uganda. In Ghana, a substantial reduction in the number of cases is expected as a result of efforts begun in 2002. In Sudan, the ongoing civil war remains the greatest obstacle to eradicating dracunculiasis (6). Negotiating an end to the war is essential for progress toward disease eradication to be achieved. In those countries in which the incidence of endemic dracunculiasis has declined substantially, the most formidable obstacles to disease eradication are apathy and complacency. To help address these obstacles, the Carter Center is beginning a media campaign to publicize the DEP campaign's accomplishments and the remaining challenges for key audiences in countries in which the disease is endemic and the international community. More information about the eradication campaign is available at http://www.cartercenter.org and http://www.cdc.gov/ncidod/dpd/parasites/guineaworm. References
* Major program partners include the ministries of health in 20 countries in which dracunculiasis is or was endemic, The Carter Center, United Nations Children's Fund (UNICEF), World Health Organization, Bill and Melinda Gates Foundation, other bilateral and private donors, U.S. Peace Corps, and CDC.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 9/18/2003 |
|||||||||
This page last reviewed 9/18/2003
|