 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Diabetes Among Young American Indians --- Montana and Wyoming, 2000--2002Type 2 diabetes is increasing among young American Indians (AIs) and other populations (1--4), and accurate surveillance is important to monitor trends in diabetes prevalence. The Indian Health Service (IHS) patient database has been used to identify cases of diabetes and estimate diabetes prevalence among AIs aged >15 years (5). However, limited studies have assessed the use of health databases to ascertain diabetes cases in young persons. The Montana Department of Public Health and Human Services (MDPHHS), in collaboration with the Billings Area IHS, conducted a study to assess use of the IHS patient database to identify AIs aged <20 years with diabetes in Montana and Wyoming. This report summarizes the results of that study, which found that diabetes cases were identified more accurately by using at least two patient visits for diabetes rather than only one patient visit. To reduce misclassification of diabetes, health-care systems and managed care organizations that use patient databases for diabetes surveillance should evaluate the accuracy of case ascertainment periodically and ensure adequate training for staff responsible for coding health-care visits and database entry. During 2000--2002, AIs aged <20 years with at least one outpatient visit or hospitalization coded for diabetes (i.e., using International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM-CM] codes 250.0--250.9) at one of six IHS facilities were identified from the IHS database. Medical records of each person were reviewed to confirm the diagnosis and classify the type of diabetes (6). MDPHHS collected demographic and clinical data and assessed the diagnoses of diabetes. A case of confirmed diabetes was defined as a case with documented diagnostic blood glucose values (7) or a record of treatment with antidiabetic therapies (e.g., insulin or oral medication). To assess the accuracy of case ascertainment, the study compared the percentage of false positives (i.e., for which persons were determined not to have diabetes) for cases based on only one health-care visit with the percentage for cases based on at least two health-care visits during 2000--2002. Diagnostic codes or reason-for-visit narratives that might have led to case misclassification were identified for the false-positive cases. The study identified 93 persons classified with diabetes based on one coded health-care visit. Assessment of the diagnoses by MDPHHS found that 40 persons (43%) did not have diabetes. No statistically significant differences by sex or by mean age were found when confirmed cases were compared with false positives. Wide variation was observed in the proportion of false-positive cases across the six clinical facilities: 0%, 25%, 27%, 50%, 67%, and 89%. Among the false-positive cases, the most common reason (15 cases out of 40) for a health-care visit was diabetes screening or a school health assessment; for 19 of the cases, no specific reason was identified (Table). On the basis of the 93 database cases with one coded health-care visit, the prevalence of diabetes in young AIs was 4.0 per 1,000 population (estimated population of AIs aged <20 years = 23,035) (8), and 2.3 per 1,000 population by using only the 53 confirmed cases. On the basis of two health-care visits, the study identified 61 persons classified with diabetes; 12 (20%) were false positives. Once again, no statistically significant differences by sex or by mean age were found. Of the 12 persons with false-positive cases, seven had been referred for a health-care visit through diabetes screening or a school health assessment. On the basis of the 61 database cases with at least two coded visits, the prevalence of diabetes in young AIs was 2.9 per 1,000 population, and 2.1 per 1,000 population by using only the 49 confirmed cases. Reported by: KR Moore, MD, Billings Area Indian Health Svc, Billings; TS Harwell, MPH, JM McDowall, CS Oser, MPH, SD Helgerson, MD, D Gohdes, MD, Montana Dept of Public Health and Human Svcs. NR Burrows, MPH, Div of Diabetes Translation, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:Accurate surveillance of type 1 and type 2 diabetes in young persons is important to monitor trends in prevalence and incidence. The findings in this report suggest that using only one ICD-9-CM coded visit during a 3-year period to ascertain diabetes cases among young AIs was accurate in only 57% of cases; therefore, the number of cases was probably overestimated by approximately 40%. The use of at least two ICD-9-CM coded visits for case ascertainment was substantially more accurate (80%). Because of the low national prevalence of diabetes in young AIs (less than five cases per 1,000 persons) (3), an increase in false-positive cases has little effect on the estimated rates; however, the number of affected young persons will be overestimated. The findings in this report are subject to at least one limitation. This analysis included only six IHS facilities. The accuracy of case ascertainment in other IHS areas and facilities might vary by facility and by the prevalence of disease in young persons. Patient databases have been useful for monitoring diabetes care in adults and can be helpful in monitoring diabetes prevalence in adolescents (5,9,10). This report highlights the importance of evaluating the use of patient databases for ascertaining diabetes cases among young persons and emphasizes the need to update and maintain case registries based on patient databases. In addition, adequate training of staff responsible for coding and database entry of patient diagnoses, particularly related to diabetes screening and school health assessments, probably will reduce misclassification of diabetes in young persons. References
Table 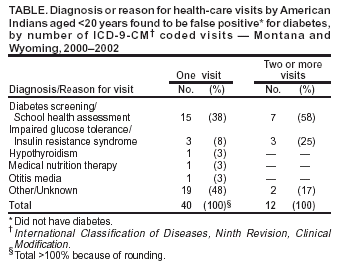 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 11/20/2003 |
|||||||||
This page last reviewed 11/20/2003
|