|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
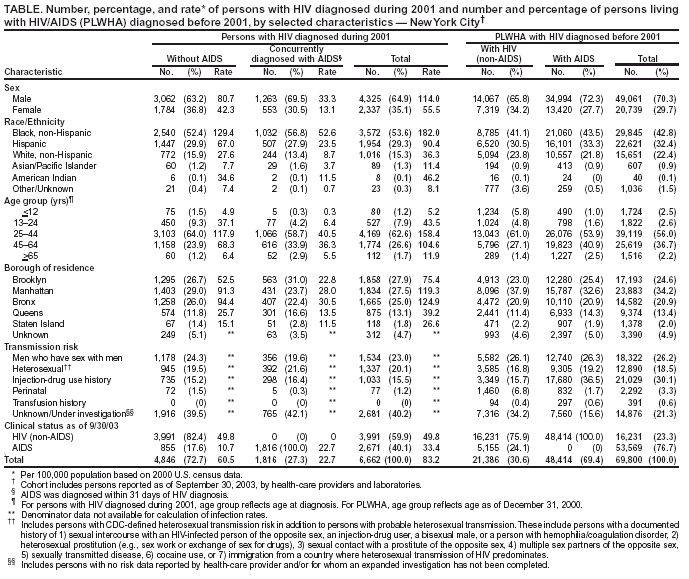
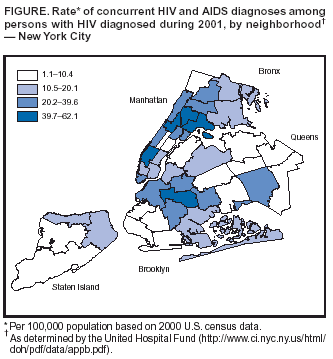
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Implementation of Named HIV Reporting --- New York City, 2001Since 1981, population-based surveillance data on acquired immunodeficiency syndrome (AIDS) have been used in New York City (NYC) to monitor the human immunodeficiency virus (HIV) epidemic. In June 2000, the NYC Department of Health and Mental Hygiene (NYCDOHMH) began tracking diagnoses of HIV (non-AIDS) in addition to AIDS diagnoses. This report describes epidemiologic data from the first full calendar year of named HIV reporting in NYC. The findings indicate that, compared with persons living with AIDS (PLWA), persons who had HIV diagnosed during 2001 were more likely to be female, non-Hispanic black, younger (i.e., aged <45 years), and residents of the Bronx or Brooklyn. These newly available data describe the NYC population with HIV infection more accurately than data on PLWA and can be used to redirect HIV-prevention efforts to better target persons at highest risk for acquiring HIV infection. A New York State (NYS) law implemented on June 1, 2000, mandates that health-care providers report by name all persons with newly diagnosed HIV infection, HIV illness, or AIDS. The law also requires that laboratories report the results of selected HIV-related tests for all NYS residents, including positive Western blot (WB) tests, detectable HIV viral loads, and CD4 counts of <500 cells/µL. NYCDOHMH field staff review medical records to abstract additional data that are not reported routinely by laboratories (e.g., race/ethnicity, transmission risk, and postal code of residence). Persons with HIV and AIDS also are identified through other mechanisms, including passive provider reporting; active surveillance by field staff in 73 acute-care hospitals, 500 clinics, and 1,500 private health-care providers' offices; and searches of public health registries (e.g., vital statistics, tuberculosis, and cryptosporidiosis). All previously unreported cases are entered into the HIV/AIDS Reporting System (HARS). NYCDOHMH analyzed surveillance data related to HIV and AIDS cases reported through September 30, 2003. Patients were categorized as having had HIV diagnosed during or before 2001 on the basis of the date of the earliest known HIV diagnostic event (e.g., WB test or Provider Report Form). Persons with HIV diagnosed during 2001 were classified further as diagnosed concurrently with HIV and AIDS if an AIDS-defining event had occurred within 31 days of HIV diagnosis. As of September 30, 2003, NYCDOHMH had received reports of 6,662 persons who had HIV diagnosed during 2001 (4,846 [73%] without AIDS and 1,816 [27%] with AIDS) (Table). An additional 3,275 persons with previously diagnosed HIV infection had AIDS diagnosed during 2001, for a total of 5,091 AIDS diagnoses during 2001. As of December 31, 2001, a total of 76,462 persons were reported to have had HIV or AIDS diagnosed and were known to be living with HIV in NYC (51,085 PLWA and 25,377 persons living with HIV [non-AIDS]). Among the 6,662 persons who had HIV diagnosed during 2001, a total of 4,325 (65%) were male, and 2,337 (35%) were female (rate ratio [RR] = 2.1; 95% confidence interval [CI] = 2.0--2.2). Non-Hispanic blacks accounted for 54% (n = 3,572; rate: 182 per 100,000 population) of HIV diagnoses (RR = 5.0; 95% CI = 4.7--5.4 compared with non-Hispanic whites); Hispanics, 29% (n = 1,954; rate: 90 per 100,000 population; RR = 2.5; 95% CI = 2.3--2.7 compared with non-Hispanic whites); and non-Hispanic whites, 15% (n = 1,016; rate: 36 per 100,000 population). Of the 3,981 (60%) HIV-infected persons for whom transmission risk data were available, 1,534 (39%) were males who reported having sex with other males, 1,337 (34%) had high-risk heterosexual contact*, and 1,033 (26%) reported injection-drug use. Overall, 1,816 (27%) of the 6,662 persons with HIV diagnosed during 2001 also had AIDS. Among NYC residents, the rates of concurrent HIV and AIDS diagnoses were highest among males and non-Hispanic blacks and varied significantly by neighborhood of residence (Figure). Persons with HIV and AIDS diagnosed concurrently were more likely to be male than female (odds ratio [OR] = 1.3; 95% CI = 1.2--1.5), non-Hispanic black than non-Hispanic white (OR = 1.3; 95% CI = 1.1--1.5), and residents of boroughs other than Manhattan (Table). Compared with PLWA who had diagnoses before 2001, persons with HIV diagnosed during 2001 were more likely to be female (35% versus 28%), aged <45 years (72% versus 57%), non-Hispanic black (54% versus 44%), and residents of the Bronx (25% versus 21%) or Brooklyn (28% versus 25%). Reported by: D Nash, PhD, C Ramaswamy, MPH, HIV Surveillance and Epidemiology Program, Bur of HIV/AIDS, New York City Dept of Health and Mental Hygiene, New York. S Manning, MD, EIS Officer, CDC. Editorial Note:Surveillance data from the first full calendar year of named HIV reporting in NYC reflect trends in HIV transmission that would not be discernable by tracking AIDS cases alone and can be useful in guiding the distribution of HIV-treatment resources. Persons with newly diagnosed HIV infection are more likely to be female, non-Hispanic black, younger (i.e., aged <45 years), and residents of the Bronx or Brooklyn. These data can be used for prevention planning activities, policy-making, and allocation of HIV-prevention resources (e.g., the annual allocation of approximately $45 million in federal, state, and local HIV-prevention funds and $103 million in Ryan White treatment funds). The proportion of persons in NYC with HIV and AIDS diagnosed concurrently (27%) is comparable to the estimated 26% concurrent HIV/AIDS diagnoses in 25 U.S. states with HIV reporting (1). Because earlier diagnosis leads to earlier initiation of treatment, delay in the progression of HIV disease, and limitation of the spread of HIV, persons in neighborhoods and risk groups with higher rates of concurrent HIV/AIDS diagnoses should be targeted for increased testing. The findings in this report are subject to at least four limitations. First, the initiation of HIV reporting in NYC resulted in a large increase in the number of persons reported with HIV and AIDS. Ascertaining transmission risk for a substantial proportion of these persons has not been possible; no transmission risk data were available for approximately 40% of those who received diagnoses during 2001. For this reason, available transmission risk data cannot be generalized to all persons with HIV infection. To address this limitation, in April 2002, NYCDOHMH, in collaboration with CDC, implemented a systematic sampling approach to obtain transmission risk data for a representative sample of persons reported with HIV, stratified by borough and sex, retroactive to June 2000 (2). Second, the completeness of HIV (non-AIDS) case reporting is not known. During 1993, completeness of AIDS case reporting in NYC was approximately 81%--87% (3), and AIDS surveillance data probably accurately reflect the actual burden of AIDS. However, surveillance data regarding HIV (non-AIDS) might underestimate the number of persons with HIV infection (non-AIDS) diagnosed. Third, persons with undiagnosed HIV cannot be detected by the HIV/AIDS surveillance system. An estimated 25% of persons living with HIV infection have never been tested, are unaware of their HIV-infection status, and are not counted by surveillance systems (4). Finally, the number of new HIV diagnoses in NYC during 2001 might be overestimated because of repeat WB testing among persons with HIV (non-AIDS) diagnosed before the start of HIV reporting. For this reason, the analysis was restricted to the first full calendar year of HIV reporting. The addition of epidemiologic data related to persons with HIV (non-AIDS) to the HIV/AIDS surveillance system in NYC has resulted in a more complete and accurate characterization of the HIV epidemic. This new epidemiologic information, coupled with proven prevention strategies, will allow for more precise targeting of HIV-prevention resources in NYC. Acknowledgments This report is based on data provided by L Jones, D Figueroa, S Ly, R Shum, T Singh, S Forlenza, J Sackoff, L Torian, M Pfeiffer, M Katyal, Y Bennani, R Quintyne, G Bramble, R Castellan, W Davis, R Evans, V Gibbs, S Lashley, P McNamee, G Pruitt, P Rosas, W Smith, C Storck, D Thompson, A Torbert, V Peters, A Brooks, C Mapson, HIV Surveillance and Epidemiology Program, Bur of HIV/AIDS; P Thomas, Div of Epidemiology, New York City Dept of Health and Mental Hygiene, New York. R Dicker, Epidemiology Program Office; M McKenna, National Center for HIV/AIDS, STD, and TB Prevention, CDC. References
* Includes persons with CDC-defined heterosexual transmission risk in addition to persons with probable heterosexual transmission. These include persons with a documented history of 1) sexual intercourse with an HIV-infected person of the opposite sex, an injection-drug user, a bisexual male, or a person with hemophilia/coagulation disorder, 2) heterosexual prostitution (e.g., sex work or exchange of sex for drugs), 3) sexual contact with a prostitute of the opposite sex, 4) multiple sex partners of the opposite sex, 5) sexually transmitted disease, 6) cocaine use, or 7) immigration from a country where heterosexual transmission of HIV predominates.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 12/30/2003 |
|||||||||
This page last reviewed 12/30/2003
|