 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Congenital Syphilis --- United States, 2002Congenital syphilis (CS) occurs when the spirochete Treponema pallidum is transmitted from a pregnant woman with syphilis to her fetus. Untreated syphilis during pregnancy can lead to stillbirth, neonatal death, or infant disorders such as deafness, neurologic impairment, and bone deformities. This report summarizes 2002 CS surveillance data, which indicated that CS rates have decreased among all racial/ethnic minority populations and in all regions of the United States except the Northeast. To further decrease CS, collaborative efforts among health-care providers, health insurers, policymakers, and the public are needed to increase prenatal care and syphilis screening during pregnancy for women at risk for delivering infants with CS. CDC analyzed national surveillance data for CS cases* reported to state and local health departments in 2002. Rates of CS per 100,000 live-born infants were determined from U.S. natality data†. During 2000--2002, the rate of CS decreased 21.1%, from 14.2 to 11.2 cases per 100,000 live births, and primary and secondary (P&S) syphilis rates among women declined 35.3%, from 1.7 to 1.1 cases per 100,000 women; cases of CS decreased from 578 cases in 2000 to 451 cases in 2002. The declines in CS rates among infants and P&S syphilis rates among women during 2000--2002 continue a pattern observed during the 1990s; CS rates and P&S syphilis rates among women have declined every year since 1991 (Figure 1). During 2000--2002, the rate of CS declined in all racial/ethnic minority populations in the United States. The rate of CS declined 50.6% among American Indian/Alaska Native infants, 22.4% among Hispanic infants, 21.4% among Asian/Pacific Islander infants, and 19.8% among non-Hispanic black infants; the rate remained unchanged among non-Hispanic white infants (Table). In addition, rates of CS declined in all regions§ of the United States except the Northeast. The rate of CS declined 29.5% in the South, 22.9% in the West, and 12.5% in the Midwest; the rate increased 0.9% in the Northeast (Table). In 2002, CS cases were reported from 138 (4.4%) of the 3,139 U.S. counties; in 2000, cases were reported from 170 (5.4%) counties. Among the 451 cases of CS reported in 2002, a total of 333 (73.8%) occurred because the mother had no documented treatment or received inadequate treatment of syphilis before or during pregnancy (Figure 2); many of these cases occurred among infants born to women who had no prenatal care or no documented prenatal care. In 63 (14.0%) cases, the mother was treated adequately but did not have an adequate serologic response to therapy, and the infant was evaluated inadequately for CS. In 39 (8.6%) cases, the mother was treated adequately but did not have an adequate serologic response to therapy, and the infant's evaluation revealed laboratory or clinical signs of CS. A total of 16 (3.6%) cases were reported for other reasons. In 288 (63.9%) CS cases reported in 2002, the mother received prenatal care; the mother did not receive prenatal care in 130 (28.8%) cases, and no information on prenatal care was reported for 33 (7.3%) cases. Use of prenatal care by mothers of infants with CS did not differ substantially in 2002 compared with 2000 (1). In 2002, the trimester when the first prenatal visit occurred could be determined for 238 (82.6%) of the 288 mothers who received prenatal care; 86 initiated care during the first trimester of pregnancy, 93 during the second trimester, and 59 during the third trimester. A total of 18 (30.5%) mothers who initiated prenatal care during the third trimester did so <30 days before delivery. In 2002, among infants with CS, 18 (4.0%) were stillborn, and eight (1.8%) died within 30 days of delivery. Reported by: AO Edozien, Assoc of Teachers of Preventive Medicine, Univ of North Carolina, Chapel Hill, North Carolina. JD Heffelfinger, MD, HS Weinstock, MD, SM Berman, MD, S Clanton, Div of STD Prevention, National Center for HIV, STD, and TB Prevention, CDC. Editorial Note:Decreases in CS rates closely parallel decreases in P&S syphilis rates among women, and interventions designed to prevent, detect, and treat syphilis among women of reproductive age likely have played an important role in the decline of CS rates. In 1998, efforts to eliminate syphilis were initiated in the United States, and prevention of CS was a key objective of the National Plan to Eliminate Syphilis, which was launched the following year (2). Elimination efforts initially focused on syphilis among racial/ethnic minority populations and persons living in the South, two populations with the highest CS and P&S syphilis rates. Although rates of CS are still substantially higher among infants born to women in racial/ethnic minority populations, declines in CS rates have been greatest among minority women and women living in the South. Early detection and treatment of syphilis among women before or during pregnancy are integral to reducing rates of CS. Syphilis elimination activities that might have reduced the occurrence of CS include 1) enhanced screening of women at high risk for acquiring syphilis, 2) efforts to increase provider awareness, education, and training regarding syphilis, and 3) efforts to increase awareness of the disease among communities with high rates of infection. Although the rate of CS declined 63.3% during 1997--2002, rates of P&S syphilis have increased recently among men, particularly men who have sex with men (3), and enhanced national and local prevention efforts have been directed toward this population. Continued progress toward reducing CS will require that syphilis elimination efforts among women of reproductive age be maintained. Ensuring that all women receive prenatal care and are screened for syphilis during pregnancy will reduce the incidence of CS. Lack of prenatal care and late or limited prenatal care continue to be important factors associated with CS (4,5). In 2002, a total of 29% of mothers of infants with reported CS did not receive prenatal care, and fewer than half of mothers who did receive prenatal care initiated it during their first trimester of pregnancy. Inadequate health-care provider adherence to CS screening recommendations also can result in CS. In a 1999--2000 national survey, 14% of obstetricians/gynecologists did not report routinely screening pregnant women for syphilis (6), and many providers who do screen for syphilis do so only once during pregnancy. CDC recommends more frequent testing among pregnant women at high risk (e.g., uninsured women, women living in poverty, sex workers, and illicit drug users) or those who live in areas of excess syphilis morbidity (7). In some counties with a high incidence of syphilis, only 16% of mothers had at least two documented prenatal syphilis tests, and only 46% had a documented syphilis test at delivery (8). The findings in this report are subject to at least three limitations. First, because the quality of surveillance data varies at local and state levels, case definitions might have been applied inconsistently in some areas. Second, because of difficulties in diagnosing CS in asymptomatic infants who were exposed to syphilis in utero, reporting of asymptomatic CS cases might be incomplete. Finally, because of difficulties in obtaining medical records during case investigations, maternal treatment history and infant laboratory data reporting were incomplete. Although the incidence of CS has decreased substantially since implementation of syphilis elimination activities, the majority of CS cases reported in 2002 were preventable. Community-based organizations, health-care providers, and government organizations can assist in preventing CS by collaborating to promote access to and use of comprehensive prenatal care for women who are uninsured or who are covered by public insurance programs (e.g., Medicaid). In addition, the findings in this report underscore the need to improve prenatal health-care providers' adherence to screening and treatment practices for pregnant women and to address socioeconomic factors associated with syphilis. Ongoing efforts to form and maintain coalitions developed to eliminate syphilis can assist in decreasing the prevalence of syphilis among women of reproductive age and the incidence of CS. Acknowledgment The data in this report are based on contributions by state and local health departments. References
* A case of CS was defined in a live-born infant who 1) had a reactive treponemal serologic test for syphilis and evidence of CS on physical examination, radiologic test, or cerebrospinal fluid (CSF) test; 2) had a reactive fluorescent treponemal antibody absorbed--19S-IgM antibody test or IgM enzyme-linked immunosorbent assay; 3) had T. pallidum identified from external lesions, placenta, umbilical cord, or autopsy specimens, or whose mother had a syphilitic lesion at delivery; 4) was born to a woman with untreated or inadequately treated syphilis before or during pregnancy; or 5) was born to a woman with syphilis whose serologic response to penicillin therapy was not documented or was documented to be inadequate (i.e., less than a fourfold decline in nontreponemal serologic titer) and had either a radiologic and/or CSF test consistent with CS or did not undergo a radiologic and/or CSF examination for signs of syphilis. The definition also included stillbirths among women with untreated syphilis. † From the National Center for Health Statistics' vital statistics natality tapes for 1989--2002. Available at http://www.cdc.gov/nchs/births.htm. § Northeast : Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont; Midwest : Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin; South: Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, and West Virginia; and West : Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming.
Figure 1 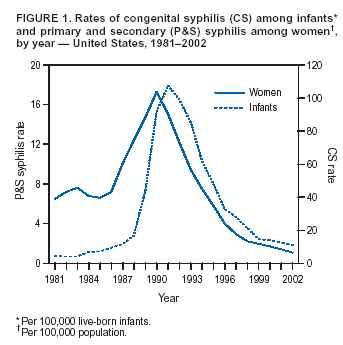 Return to top. Figure 2 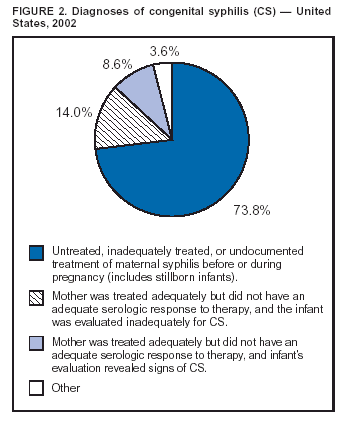 Return to top. Table 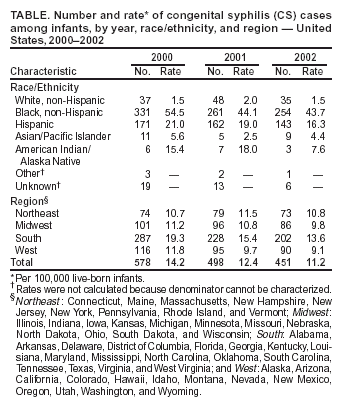 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 8/12/2004 |
|||||||||
This page last reviewed 8/12/2004
|