|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
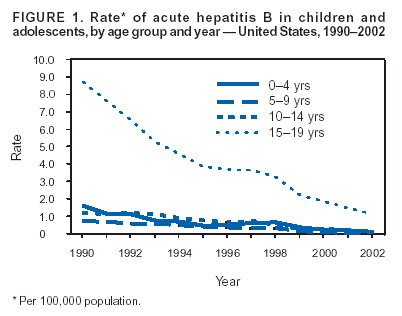
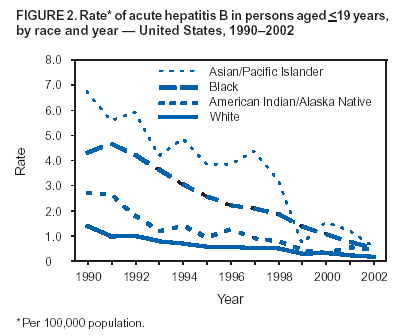
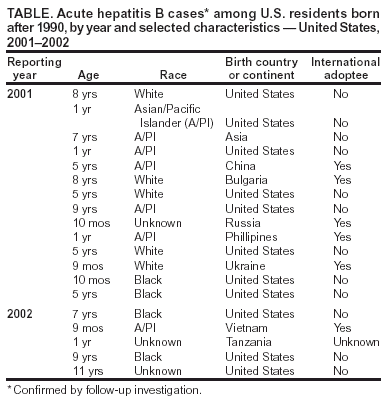
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Acute Hepatitis B Among Children and Adolescents --- United States, 1990--2002Since the 1991 adoption of a comprehensive strategy to eliminate hepatitis B virus (HBV) transmission in the United States (1), the incidence of acute hepatitis B cases has declined steadily. Declines have been greatest among children born after the 1991 recommendations for universal infant hepatitis B vaccination were implemented. In 1995, the elimination strategy was expanded to include routine vaccination of all adolescents aged 11--12 years and, in 1999, to include children aged <18 years who had not been vaccinated previously (2). To describe the epidemiology of acute hepatitis B in children and adolescents in the United States, CDC analyzed notifiable disease surveillance data collected during 1990--2002 and data collected during 2001--2002 through enhanced surveillance of reported cases of acute hepatitis B in children born after 1990. This report summarizes the results of that analysis, which indicated that the rate of acute hepatitis B in children and adolescents decreased 89% during 1990--2002 and that racial disparities in hepatitis B incidence have narrowed. Many confirmed cases in persons born after 1990 occurred among international adoptees and other children born outside the United States. Continued implementation of the hepatitis B elimination strategy and accurate surveillance data to monitor the impact of vaccination are necessary to sustain the decline of acute hepatitis B among children. Cases of acute hepatitis B were reported weekly to CDC by all 50 states and the District of Columbia. Acute hepatitis B rates were calculated per 100,000 population by using population denominators from the U.S. Census Bureau. Acute hepatitis B was defined as an acute illness with 1) discrete onset of symptoms and jaundice or elevated serum aminotransferase levels and 2) laboratory evidence of either IgM antibody to hepatitis B core antigen (IgM anti-HBc) or hepatitis B surface antigen (HBsAg). Since March 2001, CDC has conducted enhanced hepatitis B surveillance, contacting states to confirm all reported cases of acute hepatitis B in persons born after 1990. State surveillance staff members were asked to verify each of the items in the case definition and provide information regarding vaccination history and country of birth. If errors were identified during this process, states were asked to correct the information in an updated submission to CDC. National SurveillanceDuring 1990--2002, a total of 13,829 cases of acute hepatitis B were reported in the United States among persons aged <19 years. The incidence of reported cases declined steadily during this period, from 3.03 per 100,000 population in 1990 to 0.34 in 2002, representing a decline of 89%. The incidence among adolescents aged 15--19 years was consistently higher than the incidence among younger age groups (Figure 1), ranging from 8.69 per 100,000 population in 1990 to 1.13 in 2002. Children and adolescents in all age groups experienced steep declines in incidence during 1990--2002; incidence declined 94% among children aged 0--4 years, 92% among children aged 5--9 years, 93% among those aged 10--14 years, and 87% among adolescents aged 15--19 years. Among children and adolescents aged <19 years in 1990, incidence per 100,000 population was highest among Asian/Pacific Islanders (A/PIs) (6.74) and blacks (4.29); whites had the lowest race-specific incidence (1.39). Differences in incidence between whites and A/PIs and between whites and blacks were 5.34 and 2.90, respectively. From 1990 to 2002, rates declined 92% among A/PIs, 88% among whites, 88% among blacks, and 84% among American Indians/Alaskan Natives (AI/ANs) (Figure 2). In 2002, the highest incidence per 100,000 population was among A/PIs (0.55), followed by blacks (0.51), AI/ANs (0.43), and whites (0.16); since 1990, differences in incidence between whites and A/PIs and whites and blacks declined by 93% and 88%, respectively. Case InvestigationsFollow-up investigations conducted by CDC and state and local health departments verified 19 case reports from 2001 and 2002 as cases of acute hepatitis B among children born after 1990 (Table). Of the verified case reports, 12 (60%) involved males, eight (42%) involved children aged <2 years, and 11 (58%) involved children born in the United States. Seven (37%) reported race as A/PI, five (26%) as white, four (21%) as black, and three (16%) as unknown. Eight (42%) cases were reported in children born outside the United States, including six international adoptees (32%). Receipt of >1 dose of hepatitis B vaccine was confirmed in three (16%) cases. Vaccination status was unknown for 12 cases (63%). Reported by: State and local health departments. C Shepard, MD, L Finelli, DrPH, B Bell, MD, J Miller, MPH, Div of Viral Hepatitis, National Center for Infectious Diseases, CDC. Editorial Note:The incidence of acute hepatitis B cases in U.S. children and adolescents decreased during the era of universal childhood vaccination. This decline coincided with an increase in hepatitis B vaccination coverage among children aged 19--35 months, from 16% in 1992 to 90% in 2002, and among adolescents aged 13--15, from nearly 0 in 1992 to 67% in 2002 (3,4). Declines in incidence were observed for children of all races, including A/PIs, whose rates historically have been higher than the national average. Because of the disproportionate burden of hepatitis B in A/PI communities, A/PI children were among the first groups for whom hepatitis B vaccination was recommended (3). The reduction of the disparity between A/PIs and other children is consistent with recent observations noting a decline in seroprevalence of HBV infection and successful implementation of routine hepatitis B vaccination among Asians who have recently immigrated to the United States (5). However, of the 11 verified cases during 2001--02 of acute hepatitis B among children born in the United States, three (27%) involved A/PIs (Table). Although the national origins of these children's household members are unknown, the substantial proportion of A/PIs suggests that horizontal transmission of HBV among first-generation Asians might be a persistent problem (6). The higher incidence among older adolescents (aged 15--19 years) likely is attributable to their having been born before universal infant hepatitis B vaccination was recommended in 1991. Incidence among older adolescents is expected to decline further as the vaccinated cohort ages and as 1999 recommendations to vaccinate all previously unvaccinated persons aged 0--18 years are fully implemented. The expected decline in rates among adolescents also might be augmented by laws in 32 states requiring proof of hepatitis B vaccination before entry into middle school (7). Follow-up information obtained through surveillance of reported cases suggests that children born outside the United States, especially international adoptees, represent a substantial proportion of cases. Cases of acute hepatitis B among international adoptees might result from undervaccination and increased risk for exposure while living in areas with high prevalence of chronic HBV infection. International adoptees are exempt from U.S. regulations* that bar entry to immigrants without documentation of hepatitis B vaccination. Studies have demonstrated that international adoptees exhibit low rates of protective titers of antibodies to vaccine-preventable diseases upon arrival in the United States, including adoptees with written evidence of age-appropriate vaccination provided by the birth country (8,9). Appropriate evaluation and remediation of the immunization status of international adoptees has been promoted through national guidelines (10); however, the extent to which these guidelines have been implemented is unknown. Despite the decline in acute hepatitis B cases among children in the United States, the presence of confirmed cases highlights the importance of infant vaccination and timely completion of the 3-dose vaccination series. The vaccination series should be started at birth, preferably before the newborn is discharged from the hospital. Infants born to women who are HBsAg positive or who have not had prenatal HBsAg testing should receive the first fose of hepatitis B vaccine within 12 hours of birth (1). Beginning the vaccination series at birth decreases the risk for perinatal HBV transmission and predicts successful completion of the series. Although enhanced surveillance data from verified case reports suggest that international adoptees and other children born outside the United States might particularly benefit from future prevention efforts, many case reports lacked risk factor information. As the incidence of acute hepatitis B among children and adolescents declines, accurate surveillance data become increasingly important to monitor the effect of immunization recommendations. Continued efforts of local, state, and national surveillance staff to improve data quality are critical to eliminating HBV transmission in the United States. References
* U.S. Code title 8, chapter 12, subchapter II, Part II, §1182, (a)(1)(C).
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 11/4/2004 |
|||||||||
This page last reviewed 11/4/2004
|