|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
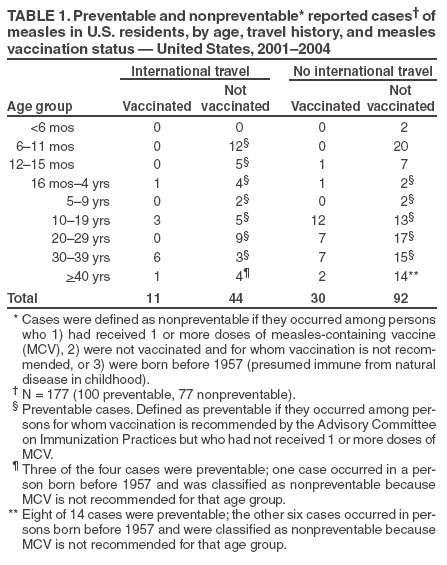
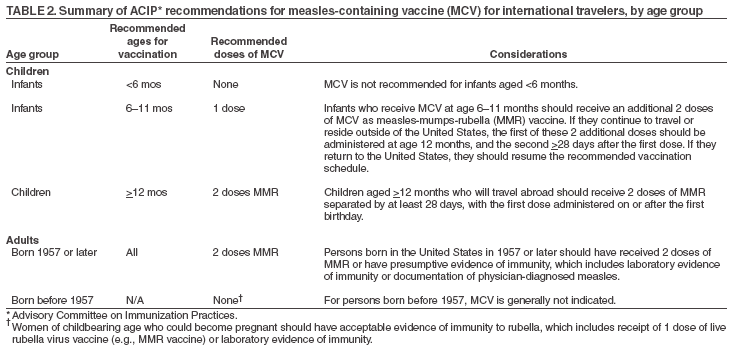
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Preventable Measles Among U.S. Residents, 2001--2004Elimination of endemic measles has been achieved in the United States (1); however, measles continues to be imported from areas of the world where the disease remains endemic, resulting in substantial morbidity and expenditure of local, state, and federal public health resources (2,3). Measles among U.S. residents results from returning residents who become infected while living or traveling abroad, from contact or association with an infected traveler, or from an unknown source. This report summarizes surveillance data reported to CDC by state and local health departments regarding confirmed measles cases among U.S. residents during 2001--2004; an illustrative case report is included. The majority of measles cases occurring among U.S. residents can be prevented by following current recommendations for vaccination, including specific guidelines for travelers (4). Confirmed measles cases (4) were defined as preventable if they occurred among persons for whom vaccination is recommended by the Advisory Committee on Immunization Practices (ACIP) but who had not received 1 or more doses of measles-containing vaccine (MCV). Cases were considered nonpreventable if they occurred among persons who 1) had received 1 or more doses of MCV, 2) were not vaccinated and for whom vaccination is not recommended, or 3) were born before 1957 (presumed immune from natural disease in childhood). Persons with unknown vaccination status were considered unvaccinated. Outbreaks were defined as three or more epidemiologically linked cases. During 2001--2004, a total of 251* measles cases were reported to CDC, of which 177 (71%) occurred among U.S. residents, and 74 (29%) occurred among nonresidents. Of the 177 cases among U.S. residents, 100 (56%) were preventable, and 77 (44%) were nonpreventable (Table 1). Preventable Cases. Of the 100 preventable cases, 43 (43%) occurred among international travelers (imported cases), and 57 (57%) among nontravelers (indigenous cases). Of the 17 (17%) preventable cases among infant travelers aged 6--15 months, 12 occurred among infants aged 6--11 months, and five occurred among children aged 12--15 months. Of the 83 (83%) preventable cases among persons aged >16 months, 26 were in persons who became infected during international travel, and 57 were in persons infected in the United States (Table 1). Nonpreventable Cases. Of the 77 cases that were nonpreventable, 12 (16%) occurred among international travelers; 11 of the 12 travelers had received at least 1 dose of MCV, and the other was born before 1957 and had not been vaccinated. A total of 65 (84%) cases occurred among nontravelers; all were in persons previously vaccinated, except 29 cases in infants aged <15 months (routine MCV may be administered as late as age 15 months) and six in persons born before 1957. Seven of the unvaccinated infants were aged 12--15 months and thus were eligible for vaccination. Outbreaks. Of the 14 outbreaks identified during 2001--2004, nine involved three or more U.S. residents; of these, seven originated with a U.S. resident traveler. In one outbreak, 10 cases in a daycare center resulted from exposure to an unvaccinated daycare attendee (an infant aged 9 months) who was infected during travel abroad (2). Case Report. During June 20--22, 2004, a North Carolina resident aged 11 years traveled from the United Kingdom to North Carolina via New York and Connecticut. After her arrival in North Carolina on June 22, she had cough, coryza, and fever, followed by onset of a rash on June 25. She had suspected measles diagnosed on June 28. She had not received MCV; her parents had declined to have her vaccinated for religious beliefs. One day before her rash onset, the girl had close contact with a male infant aged 11 months. The infant subsequently had measles with rash onset on July 4. Two days before his rash onset, the infant visited a summer camp, where he potentially had contact with up to 234 persons, including 113 campers, 63 parents/visitors, and 58 staff members. Several campers returned home at the end of the camp session, the day after the exposure. Multistate and multinational investigation and control efforts to prevent further spread were conducted. Potentially infected persons subsequently traveled to Arizona, Arkansas, Florida, New York, Australia, Costa Rica, New Zealand, South Africa, and Wales. No additional cases of measles were subsequently identified. Reported by: S Smith, North Carolina Dept of Health and Human Svcs. F Averhoff, MD, S Redd, Epidemiology and Surveillance Div, National Immunization Program; A Rue, MPH, EIS Officer, CDC. Editorial Note:Travel anywhere outside of the United States, including to industrialized regions such as Western Europe, presents a risk for measles exposure. In 2003, approximately 24 million U.S. residents traveled abroad, and 40 million international visitors entered the United States (5,6). Importation of measles from foreign visitors is unavoidable because no regulations are in effect requiring vaccination of visitors. However, as other countries reduce the burden of measles, the risk of travelers bringing measles into the United States will decrease. Measles can cause serious complications and death, particularly among children aged <5 years. All U.S. residents should be vaccinated in accordance with ACIP recommendations (4), with special attention to international travelers who now account for a substantial proportion of the measles disease burden in the United States. Health-care providers who serve populations that travel should be aware of the vaccination recommendations for international travelers (7). Current measles recommendations for travelers include vaccination for infants aged 6--11 months and 2 doses of MCV for travelers aged >12 months (Table 2). Despite these recommendations, 17% of the preventable cases described in this report occurred among unvaccinated travelers aged 6--15 months. The reasons for these children not receiving MCV are unknown but might include lack of awareness among parents and health-care providers regarding recommendations for infants aged 6--11 months, refusal because of personal or religious beliefs, or lack of perceived risk, especially for children of foreign-born U.S. residents who travel to their country of origin (8,9). Imported and secondary cases among U.S. residents who refuse vaccination because of personal or religious beliefs can result in the introduction of measles into communities with other susceptible persons who share the same beliefs, thereby posing a risk for substantial spread of disease (3,10). In addition, seven cases in nontravelers aged 12--15 months might have been prevented if these children had been vaccinated as soon as they became eligible for MCV (e.g., MMR) at age 12 months. Measles cases among persons born before 1957 for whom vaccination is not recommended are rare. However, persons in this age group who travel internationally might wish to consider vaccination to minimize their risk for measles. The findings in this report are subject to at least three limitations. First, certain measles cases might have been missed or not reported to public health officials, including cases that occurred and resolved during travel abroad. Second, because information on multiple doses of MCV is collected inconsistently, persons who had received at least 1 dose of MCV were considered vaccinated, even though 2 doses are recommended for some age groups and for most international travelers (4), thus potentially underestimating the number of preventable cases. Third, preventable cases might be overestimated because vaccine efficacy is <100%, and vaccination data were missing for 30 (17%) persons. All persons with missing data were considered unvaccinated, although some might have received MCV. Because of the high infectivity and morbidity associated with measles, contact tracing is a standard public health practice and can require many hours of public health staff time and can cost thousands of dollars (3). A recent study evaluating the economic impact of an infected U.S. traveler returning from India estimated the costs of locating and vaccinating susceptible contacts at $140,000 (3). Although few cases have been associated with transmission during air travel (3; CDC, unpublished data, 2005), contact tracing of infected air travelers is particularly challenging; a person with measles can be infectious from at least 4 days before through 4 days after rash onset. To avoid outbreaks or a resurgence of measles, as occurred during 1989--1991, when approximately 55,000 cases and 120 measles-related deaths were reported in the United States (4), high population immunity and surveillance must be maintained. To prevent measles among U.S. residents, health-care providers should follow ACIP vaccination recommendations, ensuring that travelers are vaccinated, particularly infants aged 6--11 months, and that 2 doses are administered for those aged >12 months. In addition, parents should be educated about the risk for measles associated with international travel and the need for vaccination. Information on vaccination recommendations for travelers is available from CDC at http://www.cdc.gov/travel. Acknowledgments The data in this report are based on contributions by state and local health departments. References
* Data for 2004 are provisional. Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 8/24/2005 |
|||||||||
|