|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
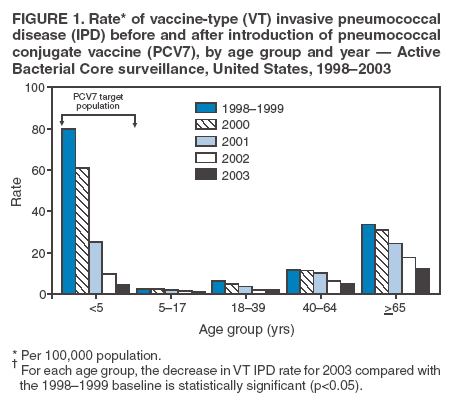
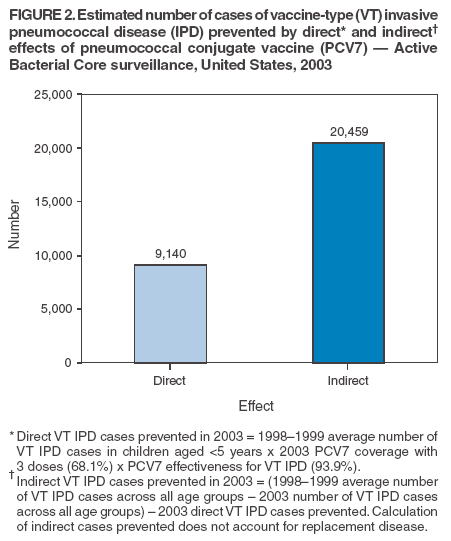
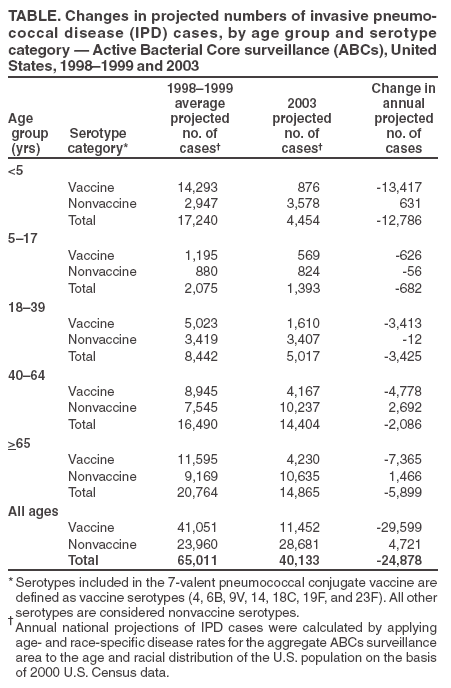
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Direct and Indirect Effects of Routine Vaccination of Children with 7-Valent Pneumococcal Conjugate Vaccine on Incidence of Invasive Pneumococcal Disease --- United States, 1998--2003Streptococcus pneumoniae (pneumococcus) is a leading cause of pneumonia and meningitis in the United States and disproportionately affects young children and the elderly. In 2000, a 7-valent pneumococcal conjugate vaccine (PCV7) was licensed in the United States for routine use in children aged <5 years (1). Surveillance data from 2001 and 2002 indicated substantial declines in invasive pneumococcal disease (IPD) in children and adults compared with prevaccine years (2,3). This report updates assessment of the impact of PCV7 on IPD through 2003 by using population-based data from the Active Bacterial Core surveillance (ABCs) of the Emerging Infections Program Network, a cooperative surveillance program conducted by several state health departments and CDC.* The results of this analysis indicated that 1) routine vaccination of young children with PCV7 continued to result in statistically significant declines in incidence of IPD through 2003 in the age group targeted for vaccination and among older children and adults, 2) the vaccine prevented more than twice as many IPD cases in 2003 through indirect effects on pneumococcal transmission (i.e., herd immunity) than through its direct effect of protecting vaccinated children, and 3) increases in disease caused by pneumococcal serotypes not included in the vaccine (i.e., replacement disease) occurred in certain populations but were small compared with overall declines in vaccine-serotype disease. Ongoing surveillance is needed to assess whether reductions in vaccine-serotype IPD are sustained and whether replacement disease will erode the substantial benefits of routine vaccination. ABCs conducted active surveillance for IPD cases through regular contact with all clinical microbiology laboratories in defined surveillance areas; periodic audits of laboratory records ensured complete case finding. Pneumococcal isolates were sent to reference laboratories for serotyping by the quellung reaction and were categorized as vaccine-type (VT) (serotypes included in PCV7) or nonvaccine-type (NT) (all other serotypes). A case of IPD was defined as isolation of pneumococcus from a normally sterile body site (e.g., blood or cerebrospinal fluid) in an ABCs area resident. Participating areas during 1998--2003 included in this analysis were the state of Connecticut and selected counties in California, Georgia, Maryland, Minnesota, New York, and Oregon, representing a total surveillance population of approximately 16 million persons in 2000. Annual incidence rates were calculated for 1998--1999 by using U.S. Census Bureau population estimates for those years; incidence rates for 2001--2003 were based on National Center for Health Statistics (NCHS) bridged-race postcensal population estimates for those years (4). For national projections of annual numbers of IPD cases, age- and race-specific rates of disease were applied from the aggregate ABCs surveillance area to the age and racial distribution of the U.S. population. The impact of PCV7 introduction on IPD was assessed in three ways. First, to assess the change in incidence of IPD after PCV7 introduction, IPD rates for 2001--2003 were compared with the average rate for 1998--1999 (baseline). Second, the projected number of VT IPD cases directly prevented by PCV7 in 2003 was calculated as the product of 1) the nationally projected number of VT IPD cases at baseline among children aged <5 years, 2) the 3-dose coverage of PCV7 in 2003 among all U.S. children aged 19--35 months identified from National Immunization Survey (NIS) data (68.1%) (5), and 3) vaccine efficacy against VT IPD from a large clinical trial (93.9%) (6). Third, the projected number of VT IPD cases indirectly prevented by PCV7 in 2003 was estimated across all ages aggregately by calculating the difference between the average annual projected number of VT cases in 1998--1999 and the projected number of VT cases in 2003, and then subtracting the number of VT cases directly prevented by the vaccine. From 1998--1999 to 2003, the incidence of VT IPD among children aged <5 years decreased from 80.0 cases per 100,000 population to 4.6, a decline of 94% (95% confidence interval [CI] = 92%--96%) (Figure 1). The total incidence of IPD (VT and NT) in this age group declined 75% (CI = 72%--78%), from 96.7 at baseline to 23.9 in 2003. Incidence rates of VT IPD also declined substantially among persons outside of the PCV7 target population (Figure 1). For persons aged >5 years, VT disease decreased 62% (CI = 59%--66%) from 1998--1999 to 2003, with the largest absolute rate reduction occurring among those aged >65 years (rate difference: 21.7 cases per 100,000 [rate 33.6 during 1998--1999 and 11.9 during 2003]). Total IPD incidence declined 29% (CI = 25%--33%), again with the majority of the absolute rate reduction occurring among those aged >65 years (rate difference: 18.4 cases per 100,000 [rate 60.1 during 1998--1999 and 41.7 during 2003]). The incidence of IPD caused by the 16 serotypes included in the 23-valent polysaccharide pneumococcal vaccine (PPV23) and not in PCV7 among persons aged >5 years increased 11% (CI = 3%--21%) from 1998--1999 to 2003. Analysis of the projected 29,599 VT IPD cases prevented nationally by PCV7 in 2003 compared with 1998--1999 (Table) revealed that the majority (69%) of cases were prevented through indirect effects of the vaccine. An estimated 9,140 cases of VT IPD were directly prevented by vaccinating children aged <5 years with PCV7; an additional 20,459 cases of VT IPD were prevented through indirect effects of the vaccine across all ages (Figure 2). Incidence of IPD caused by pneumococcal serotypes not included in PCV7 increased among children aged <5 years and adults aged >40 years, with a total of 4,721 projected additional cases of NT IPD in 2003 compared with the 1998--1999 baseline (Table). After accounting for this increase, 24,878 net cases of IPD were prevented in 2003; net prevented cases were evenly distributed between the age group targeted for vaccination with PCV7 (12,786 prevented cases [51%]) and older children and adults outside the target population (12,092 prevented cases [49%]) (Table). Reported by: A Reingold, MD, California Emerging Infections Program, Oakland, California. J Hadler, MD, Emerging Infections Program, Connecticut Dept of Public Health. MM Farley, MD, Georgia Emerging Infections Program, Veterans Affairs Medical Center and Emory Univ School of Medicine, Atlanta, Georgia. L Harrison, MD, Maryland Emerging Infections Program, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland. R Lynfield, MD, J Besser, MS, Minnesota Dept of Health. N Bennett, MD, Monroe County Dept of Public Health, Rochester, New York. A Thomas, MD, Oregon Dept of Human Svcs. W Schaffner, MD, Tennessee Emerging Infections Program, Vanderbilt Univ Medical Center, Nashville, Tennessee. B Beall, PhD, Streptococcus Laboratory; T Pilishvili, MPH, Office of Surveillance, Active Bacterial Core surveillance/Emerging Infections Program Network; CG Whitney, MD, M Moore, MD, Div of Bacterial and Mycotic Diseases, National Center for Infectious Diseases; DC Burton, MD, EIS Officer, CDC. Editorial Note:Routine use of PCV7 in young children has reduced the incidence of VT and overall IPD in children and adults, and these reductions have increased since 2001 (2). The most substantial decline in the rate of VT disease has been in the target population of children aged <5 years. Data from 2003 also demonstrate statistically significant reductions in the rates of both VT IPD and total IPD for children aged 5--17 years, whereas no statistically significant change in disease rate was observed among persons aged 5--19 years in 2001 (2). As of 2003, the total incidence of IPD in persons aged >65 years declined to 41.7 cases per 100,000 population in ABCs surveillance areas, meeting the Healthy People 2010 objective of no more than 42 cases per 100,000 for this age group (7). Indirect benefits of PCV7 (i.e., cases prevented in unvaccinated persons) exceeded direct protective benefits among immunized children, with more than twice as many cases of VT IPD prevented indirectly as directly in 2003. The indirect effects of PCV7 are believed to be caused by decreased nasopharyngeal carriage of VT strains among immunized children, which results in decreased transmission to nonimmunized children and adults (i.e., herd immunity) (2,8). On the basis of this mechanism, indirect benefits from PCV7 might be expected to increase as its vaccination coverage increases. In certain populations (e.g., children aged <5 years and adults aged >40 years), the reduction in VT IPD attributable to PCV7 was partially offset by an increase in disease caused by non-VT strains. However, during 2003, the overall magnitude of this replacement disease was small compared with the reduction in VT disease. The findings in this report are subject to at least two limitations. First, secular trends cannot be excluded as a factor in the changing pattern of IPD in the United States. However, these trends would be expected to affect disease caused by all serotypes; the reductions in IPD after introduction of PCV7 have been specific to vaccine serotypes, suggesting a vaccine effect. The decline in adult IPD likely is not attributable to PPV23, given that no decline occurred in the incidence of IPD caused by serotypes included in PPV23 but not in PCV7, and given that the slight increase in vaccine coverage of PPV23 since 1998 (9) would not be expected to cause a measurable change in IPD rate. Second, the calculations of direct and indirect effects of the conjugate vaccine were based on data estimates from several sources, each with an associated margin of error; the calculations in this report provide only crude estimates of the relative magnitudes of direct and indirect vaccine effects. In addition, the number of doses of vaccine needed to provide direct protection is unknown, and partial protection might be provided by fewer than 3 doses. The robustness of the direct and indirect effects of PCV7 has important implications for cost-benefit analyses of similar vaccines in the United States and internationally. Initial estimates of cost-effectiveness for the United States (10) did not account for indirect effects and therefore underestimated the cost-effectiveness of PCV7. In addition, ongoing surveillance will be required to monitor the balance of disease reduction versus replacement in the conjugate vaccine era, particularly in vulnerable populations (e.g., the elderly and immunocompromised persons), who might be more susceptible to less virulent non-VT strains of pneumococci. Such information will be critical for determining whether the composition of conjugate vaccines should be revised or expanded over time. Acknowledgments This report is based, in part, on contributions by P Daily, MPH, G Rothrock, MPH, California Emerging Infections Program, Oakland, California. N Barrett, MPH, Emerging Infections Program, Connecticut Dept of Public Health. W Baughman, MSPH, J Howgate, MPH, C Payne, MPH, L Rainer, MPH, P Martell-Cleary, MSW, Georgia Emerging Infections Program, Veterans Affairs Medical Center and Emory Univ School of Medicine, Atlanta, Georgia. L Sanza, Maryland Emerging Infections Program, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland. C Lexau, PhD, R Danila, PhD, B Juni, MS, G Kupferschmidt, Minnesota Dept of Health. C Long, Univ of Rochester, Rochester, New York; B Anderson, D Hoefer, New York State Dept of Health. K Stefonek, MPH, Oregon Dept of Human Svcs. B Barnes, Vanderbilt Univ Medical Center, Nashville; AS Craig, MD, Tennessee Dept of Health. TH Skoff, MS, ER Zell, MStat, C Wright, Div of Bacterial and Mycotic Diseases, National Center for Infectious Diseases, CDC. References
* Available at http://www.cdc.gov/ncidod/dbmd/abcs.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 9/14/2005 |
|||||||||
|