|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
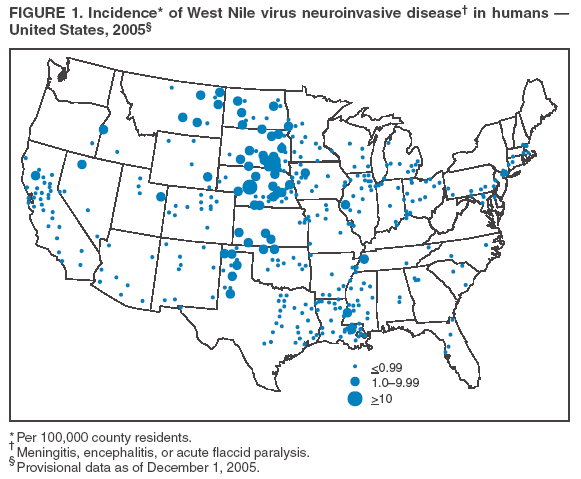
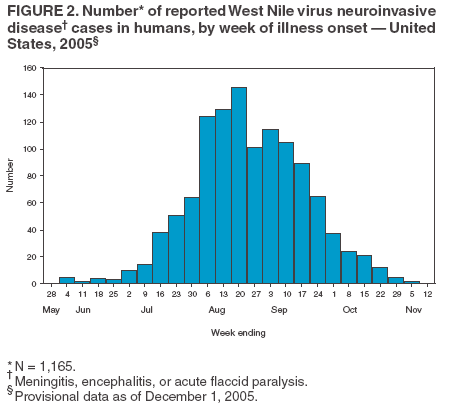
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. West Nile Virus Activity --- United States, January 1--December 1, 2005West Nile virus (WNV) is the leading cause of arboviral encephalitis in the United States. Originally discovered in Africa in 1937, WNV was first detected in the western hemisphere in 1999 in New York City. Since then it has caused seasonal epidemics of febrile illness and severe neurologic disease. During January 1--December 1, 2005, a total of 2,744 cases of WNV disease in humans* were reported in the United States, an increase from 2,359 during the same period in 2004. A total of 1,165 cases were WNV neuroinvasive disease (WNND). WNV infections in humans, birds, mosquitoes, and nonhuman mammals are reported to CDC through ArboNET, an Internet-based arbovirus surveillance system managed by state health departments and CDC. During 2005, WNV transmission to humans or animals expanded into 21 counties that had not previously reported transmission and recurred in 1,196 counties where transmission had been reported in previous years. This report summarizes provisional WNV surveillance data through December 1, 2005, and highlights the need for ongoing surveillance, mosquito control, promotion of personal protection from mosquito bites, and research into additional prevention strategies. Human SurveillanceAs of December 1, a total of 2,744 cases of WNV disease in humans had been reported from 596 counties in 42 states, 18.8% of the 3,142 U.S. counties. Among the cases, 1,165 (42.5%) were WNND (i.e., meningitis, encephalitis, or acute flaccid paralysis), 1,434 (52.2%) were West Nile fever (WNF), and 145 (5.3%) were unspecified illnesses. California reported 854 cases of WNV disease, 31% of the U.S. total, and 285 WNND cases, 25% of the U.S. total. Other focal outbreaks of WNND recurred throughout the United States, including in Illinois (133 cases), Texas (107), and Louisiana (100). In the New York City metropolitan area, WNV disease recurred for the seventh consecutive year. The highest incidence of WNND occurred primarily in the central United States (Figure 1), including South Dakota (4.8 WNND cases per 100,000 residents), Nebraska (2.1 cases per 100,000), and North Dakota (1.9 cases per 100,000). Nationally, reports of WNV disease began in late May, peaked during the third week in August, and lasted into November (Figure 2). The median age of the 1,165 persons with WNND was 57 years (range: 3 months--98 years), and 665 (57.1%) were male. A total of 994 (85.3%) persons were hospitalized, and 85 (7.3%) died. Sixty-eight (5.8%) persons with WNND had acute flaccid paralysis. Their median age was 52.5 years (range: 9--84 years), and 39 (57.4%) were male; five (7.4%) died. The median age of all persons whose deaths were related to WNND was 75 years (range: 36--98 years). The median age of the 1,434 persons with WNF was 48 years (range: 1--92 years), and 799 (55.7%) were male. A total of 325 (22.7%) persons with WNF were hospitalized, and four (0.3%) died as a result of complications; the median age of fatalities related to WNF was 89.5 years (range: 44--92 years). Animal SurveillanceA total of 5,204 dead WNV-infected birds were reported from 583 counties in 45 states; 325 counties from 43 states reported infected birds but no human disease. Collection of WNV-infected birds peaked during the third week in August. Corvids (e.g., crows, jays, and magpies) accounted for 4,274 (82.1%) of the birds; the majority of states targeted corvids for surveillance. Since 1999, WNV infection has been identified in more than 300 avian species, including 16 species with WNV identified for the first time during 2005. Of 1,089 reported WNV disease cases among nonhuman mammals, 1,072 (98.4%) occurred in equines, and 17 (1.6%) occurred in other species (dogs [five], squirrels [six], and unspecified species [six]). Equine cases were reported from 344 counties in 33 states; California reported 42% of all equine cases. Peak reported incidences of equine disease occurred during the third week in August. A total of 11,263 mosquito pools from 410 counties in 43 states and the District of Columbia tested positive for WNV. Among the WNV-positive pools, 7,224 (64.2%) were made up of Culex mosquitoes thought to be the principal vectors of WNV transmission (i.e., Cx. pipiens, Cx. quinquefasciatus, Cx. restuans, Cx. salinarius, and Cx. tarsalis) (1). Unidentified or other species of Culex mosquitoes made up 3,843 (34.1%) pools, and non-Culex species (i.e., Aedes spp., Anopheles spp., Coquillettidia spp., Culiseta spp., Ochlerotatus spp., and Psorophora spp.) made up 196 (1.7%) pools. Data from 2005 included the first report of WNV infection in Culiseta incidens. The number of reported WNV-infected mosquito pools peaked during the second week in August. Reported by: TL Smith, MD, EB Hayes, MD, DR O'Leary, DVM, RS Nasci, PhD, N Komar, ScD, GL Campbell, MD, A Hinckley, PhD, K Kniss, JA Lehman, ND Crall, LR Petersen, MD, Div of Vector-Borne Infectious Diseases, National Center for Infectious Diseases; LB Davis, DVM, EIS Officer, CDC. Editorial Note:The increase in reported cases of WNV disease in 2005 compared with 2004 suggests that endemic transmission of WNV in the United States will continue for the foreseeable future. In 2005, nearly one third of human cases were reported from California, but focal outbreaks recurred in areas where seasonal transmission has occurred for several years (1). Approximately 80% of all WNV infections are asymptomatic, approximately 20% cause WNF, and <1% cause WNND (2). The large percentage of WNND among reported cases reflects underreporting of WNF and lack of reporting of asymptomatic infections. Underreporting of WNF varies by year and geographic area. WNND has been a nationally notifiable disease since 2002. In 2005, the Council of State and Territorial Epidemiologists added WNF as a notifiable disease; however, the true incidence and public health impact of WNF remains underestimated by national surveillance data (2,3). Although persons of all ages appear equally susceptible to WNV infection, both the incidence of WNND and the incidence of death increase with age, especially among persons aged >60 years, and are slightly higher in males (1,4). During 2005, the median age among persons with fatal WNND was similar to that of previous years (4,5). Certain birds (e.g., corvids, common grackles, house finches, and house sparrows) develop high-titer WNV viremia, making them highly infectious to feeding mosquitoes. Many of these species also have high (>40%) mortality from WNV infection (1,6). Since 1999, corvids have accounted for 72% of all WNV-infected dead birds reported to CDC. The large number of reported corvid deaths likely results from their large size and susceptibility to WNV disease and death, and from surveillance programs targeted at corvids. Geographically, bird species can vary in usefulness as surveillance indicators for WNV transmission; targeting locally relevant species can optimize efficiency of WNV surveillance. Reports of WNV disease in equines have decreased annually since 2002 (CDC, unpublished data, 2005). The decline might represent a true decrease in equine disease incidence resulting from naturally acquired immunity or vaccination (7) or from less emphasis on reporting of WNV disease in equines. The 2005 temporal and geographic distribution of equine WNV cases correlated with human cases, suggesting that equine surveillance can continue to help indicate areas of increased risk for human WNV disease. The Culex species most prevalent in WNV-positive pools during 2005, Cx. pipiens, Cx. quinquefasciatus, Cx. restuans, and Cx. tarsalis, are believed to account for most WNV transmission in the United States (1). During 2005, a total of 34 different WNV-infected mosquito species were identified, including key species in the transmission of other arboviral diseases. These species include Cx. nigripalpus, the principal vector of St. Louis encephalitis (SLE) in Florida (8), and Cx. tarsalis, a major vector of SLE and western equine encephalitis in western states (8). Although other species (e.g., Aedes triseriatus, Ae. albopictus, and Ae. aegypti) might contribute to WNV transmission to humans, control of Culex mosquitoes remains critical to reducing risk for human WNV disease. In 2005, WNV spread into areas of the western United States where transmission previously was not documented; WNV has recurred annually in other regions. Ongoing WNV surveillance monitors the spread of the virus and helps target prevention and control strategies. Through increased attention to arboviral diagnosis, testing, and reporting, the ArboNET surveillance system is well positioned to detect increased transmission of all endemic arboviruses and introduction of other foreign arboviruses. In the absence of an effective vaccine, prevention of WNV disease depends on community-level mosquito control and promotion of personal protection against mosquito bites, such as use of repellents and avoiding outdoor exposure when mosquitoes are active. Acknowledgments This report is based, in part, on data provided by ArboNET surveillance coordinators in local and state health departments and ArboNET technical staff, Div of Vector-Borne Infectious Diseases, National Center for Infectious Diseases, CDC. References
* Defined using the Council of State and Territorial Epidemiologists case definition for neuroinvasive and nonneuroinvasive arboviral diseases, available at http://www.cdc.gov/epo/dphsi/print/arboviral_current.htm.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 12/15/2005 |
|||||||||
|