|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
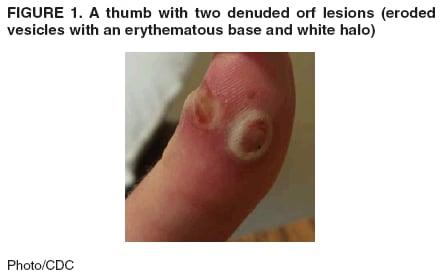
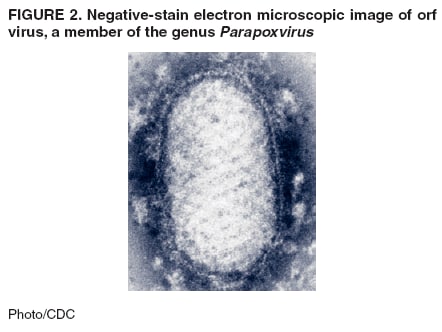
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Orf Virus Infection in Humans --- New York, Illinois, California, and Tennessee, 2004--2005Orf virus is a zoonotic parapoxvirus endemic to most countries in the world and is principally associated with small ruminants (e.g., sheep and goats). Human orf infections appear as ulcerative skin lesions after contact with an infected animal or contaminated fomite. This report summarizes the epidemiologic and laboratory investigations of four sporadic cases of human orf infection, emphasizing the temporal association between human lesions and skin trauma or recent flock vaccination with live orf vaccine. This zoonotic infection shares clinical manifestations and exposure risks with other, potentially life-threatening zoonoses (e.g., cutaneous anthrax) and is likely under-recognized because of a lack of clinical suspicion and widely available diagnostics. Barrier precautions and proper hand hygiene are recommended for the prevention of orf virus infection in humans. Case 1. On March 1, 2004, a woman aged 51 years from upstate New York noted an area of erythema approximately 4 mm in diameter on the middle finger of her right hand. During the next several days, the lesion evolved into a clear, solitary vesicle with surrounding erythema. On March 12, she visited her family physician, who prescribed penicillin and warm water soaks. The patient did not recall any trauma, including animal bites, although she regularly cared for goats on her family farm. She reported having bottle-fed a kid goat with a sore on its mouth approximately 1 week before the appearance of the lesion. The patient did not improve and, on March 15, she went to a local hospital. The lesion on her finger had progressed to 2 cm in diameter with a 3--4 mm central white ring and umbilication. Her examination was otherwise unremarkable. At the hospital, the ulcer was debrided and a serous/gelatinous material was extracted. Routine bacterial cultures were negative. The patient was treated empirically with ciprofloxacin and amoxicillin-clavulanate. On March 22, after discussion with local veterinarians, she contacted the New York State Department of Health to inquire about diagnostics for orf virus infection. Specimens collected on March 15 were forwarded to CDC and determined to be positive at both genus (Parapoxvirus) and species (orf virus) level by real-time polymerase chain reaction (PCR); standard PCR (i.e., visualization of amplicons by gel electrophoresis) (1) for genus and species was negative. By April 1, the lesion had spontaneously healed without scarring. No other family members or farm attendants reported similar skin lesions. Case 2. In May 2004, an adolescent boy aged 16 years was bitten on the left hand by a healthy-appearing sheep that he was grooming for a county fair in southwestern Illinois. The sheep had been vaccinated against orf virus 1 week before the patient was bitten. Three weeks after he sustained the bite, the patient went to his primary-care physician with three nonpruritic, painless vesicular lesions on his left thumb, the largest of which was 1.5 cm in diameter. Two lesions were eroded vesicles with an erythematous base and white halo (Figure 1); the remaining periungual lesion around the nail was still intact. The patient reported no constitutional symptoms, and the rest of his physical examination was unremarkable. Skin from the unroofed vesicle and dry swabs of material from the ulcer beds were submitted to CDC to confirm the diagnosis of orf virus infection. Both real-time PCR and standard PCR were positive in genus- and species-specific assays, confirming the diagnosis of orf virus infection. No treatment was administered, and the lesions healed spontaneously after 2 months. The sheep was removed from the county fair once the orf infection was evident, and active case finding failed to reveal other orf infections in county fair staff or attendees. Case 3. On July 28, 2004, a man aged 51 years from Sonoma County, California, was referred to an infectious diseases physician because of pruritic, painless vesicles on his left hand. He had onset of these lesions 10 days after shearing young sheep, which had been purchased recently at auction and vaccinated with the live orf vaccine. The patient noted that some of the sheep had ulcers on their oral mucosa. He also recalled cutting his skin on thistles and burs embedded in the sheep wool. He reported no constitutional symptoms. His physical examination was only remarkable for five bullae (vesicles >1 cm in diameter), 1.0--1.5 cm in diameter, on the back of both hands. A punch biopsy specimen of one lesion was sent to the Santa Rosa Kaiser Medical Center Pathology Department, and serum was submitted to the California State Health Department Laboratory for further testing. Histopathology indicated nonspecific inflammation, but serologic evaluation revealed parapoxvirus IgM >1:160 and IgG of 1:512, consistent with current or recent parapoxvirus infection. All lesions healed spontaneously within 2 weeks. Case 4. On May 25, 2005, a girl aged 11 years was taken to her pediatrician in Nashville, Tennessee, with a 7-mm papulovesicular lesion on the fourth finger of her left hand. Ten days before this visit, her family had vaccinated their sheep against orf virus. Five days before her clinic visit, she had cut the same finger on a lamb harness. The remainder of her physical examination was unremarkable. The lesion was lanced in clinic, producing 3 cc of bloody discharge that was submitted to CDC for evaluation of orf virus infection. While laboratory results were pending, the patient was treated with amoxicillin-clavulanate twice a day for 10 days. Real-time PCR performed at CDC confirmed the presence of orf virus using both genus- and species-specific primers, and standard PCR assays were negative for both primer sets. The lesion healed spontaneously within 1 month. No other family members reported similar lesions to the attending physician. Reported by: G Green, MD, Dept of Infectious Diseases, Kaiser Permanente, Santa Rosa; D Schnurr, PhD, Div of Communicable Disease Control, Viral and Rickettsial Disease Laboratory, California Dept of Health Svcs. D Knoll, MSN, Madison County Health Dept, Wood River; R Griffith, MPH, C Austin, PhD, Illinois Dept of Public Health. M Clark, Chautauqua County Dept of Health, Mayville; P Smith, MD, A Sullivan-Frohm, New York State Dept of Health. J Ragsdale, MD, Old Harding Pediatrics Hospital, Nashville, Tennessee. F Coronado, MD, Office of Workforce and Career Development; E Goldman, PhD, M Reynolds, PhD, IK Damon, MD, PhD, Y Li, PhD, V Olson, PhD, Poxvirus Program, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; ER Lederman, MD, EIS Officer, CDC. Editorial Note:Although orf virus infection is self-limiting in hosts with normal immune systems, it can resemble skin lesions associated with potentially life-threatening zoonotic infections such as tularemia, cutaneous anthrax, and erysipeloid (2); therefore, rapid and definitive diagnosis is critical. Tularemia and erysipeloid are generally associated with exposure to rabbits or New World sylvan rodents and swine, respectively. Both orf virus infection and naturally acquired anthrax in humans can result from exposure to domestic sheep and goats; thus, exposure history alone (i.e., animal contact) is insufficient to indicate etiology, necessitating laboratory evaluation. Histopathologic features include intraepithelial ballooning and intracytoplasmic inclusions (3); however, these findings are suggestive and not pathognomonic. Negative-stain electron microscopy can confirm a parapoxvirus infection by demonstrating classic ovoid cross-hatched virions (Figure 2) but cannot distinguish orf virus from other parapoxviruses such as paravaccinia (pseudocowpox) virus; serologic testing has the same limitation. Only PCR can definitively identify a parapoxvirus as orf virus. Two assays have been used by CDC: standard PCR (1) and real-time PCR. Cases 1 and 4 described in this report demonstrate the increased sensitivity of the newer real-time PCR technique (nearly 1,000 times more sensitive than standard PCR) (Y. Li, PhD, CDC, personal communication, November 2005). This high level of sensitivity has been observed for other poxvirus real-time PCR assays validated by CDC (4). These assays are ideally performed on frozen tissue specimens, vesicle material, or scab debris. Transmission of orf virus to humans occurs after contact with infected or recently vaccinated animals and/or fomites in conjunction with skin trauma. Orf virus vaccine strains have been known to cause outbreaks among sheep (5), and three of the illnesses described in this report occurred soon after vaccination of the flock. Veterinary vaccines for orf virus use nonattenuated, live virus preparations and are intended to produce controlled infections in flocks (6). Recently vaccinated animals pose an occupational risk to humans (7). Infections in three of the four cases described in this report were temporally associated with orf virus vaccination; however, the vaccines used to inoculate the animals in question were not available for genetic comparison with patient isolates. Three of the four cases described in this report were associated with concurrent skin trauma; orf virus infection is facilitated by skin trauma (8), and previous case series have associated skin trauma with orf virus infection (3). Trivial injury (e.g., pricks from thistle) or substantial trauma (e.g., bites) can facilitate transmission of orf virus. Therefore, barrier protection (e.g., nonporous gloves) and hand washing during the care of sheep and goats is recommended whenever feasible. These measures are especially important for any person with a compromised immune system or a chronic skin disorder (e.g., eczema) who has contact with overtly infected animals. Immunocompromised persons should discuss the risks of handling orf-infected animals and infection-prevention strategies with their primary-care physicians. Human orf virus infection is a common yet preventable consequence of contact with sheep and goats. Persons who are most likely to be exposed to orf virus (e.g., farm workers) might be familiar with the infection and thus might not seek medical attention. As a result, clinicians might not be familiar with orf virus infections, leading to a delay in diagnosis and unnecessary antibiotic use. Public health personnel should be cognizant that orf virus infection is similar in appearance and risk factors to life-threatening infections such as cutaneous anthrax and that skin trauma is a predisposing factor to infection. In addition, immunocompromised patients can have progressive, destructive lesions requiring medical interventions such as antiviral therapy (9) and surgical debridement (10). The relation between vaccination of sheep and goats for orf virus and subsequent human orf virus infection should be considered in future public health investigations. Barrier precautions and proper hand hygiene are recommended for the prevention of orf virus infection in humans. Upon request, definitive diagnostic testing for orf virus is available at CDC, telephone 404-639-4129. Acknowledgments The findings in this report are based, in part, on contributions by S Nuernberger, MD, D Driscoll, Anderson Hospital, Maryville; P Gabel, B Sobczak, Madison County Health Department, Wood River; CM O'Keefe, DVM, Illinois Department of Agriculture; L Byrd, MPH, K Kelly-Shannon, Illinois Department of Public Health; and J Abel, C Goldsmith, MS, Division of Viral and Rickettsial Diseases, National Center for Infectious Diseases, CDC. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 1/26/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|