|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
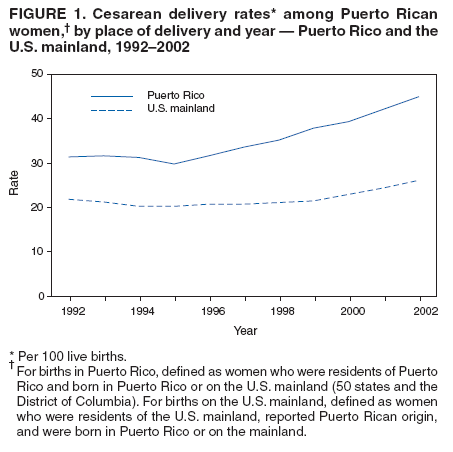
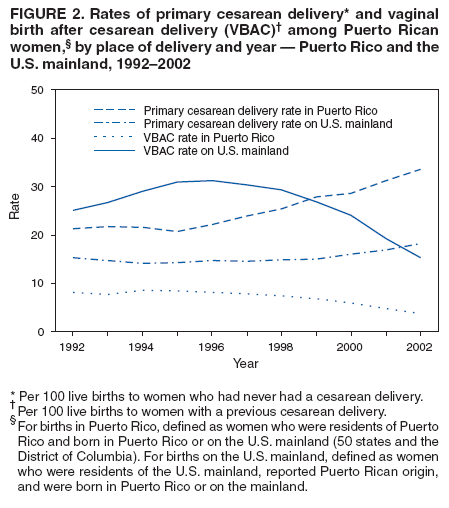
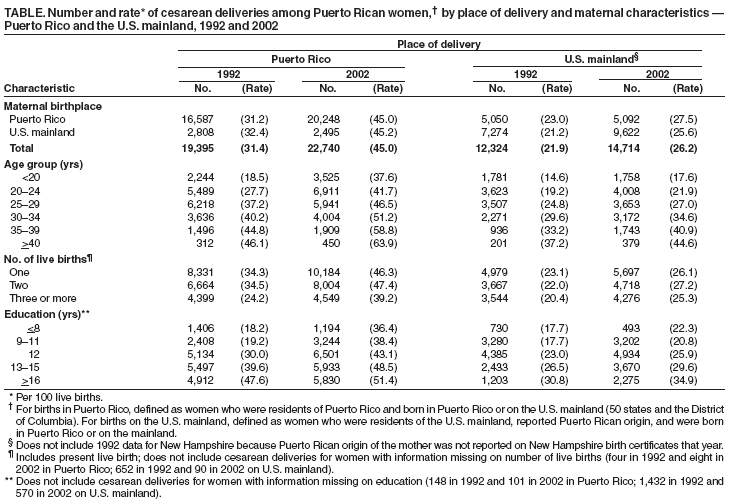
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Rates of Cesarean Delivery Among Puerto Rican Women --- Puerto Rico and the U.S. Mainland, 1992--2002Cesarean delivery has been associated with greater risks for maternal morbidity (1,2), longer hospital stays, and rehospitalization after childbirth (2,3) than vaginal delivery. On the U.S. mainland (i.e., 50 states and District of Columbia), rates of total cesarean delivery and primary cesarean delivery (i.e., for women without a previous cesarean) per 100 live births decreased from 1992 to 1996 before increasing from 1996 to 2002. During 2002, among all U.S. mainland births (approximately 4 million), 26% were by cesarean delivery; among all mainland births to women without a previous cesarean delivery, 18% were by primary cesarean (4). Cesarean delivery rates for Puerto Rican women who delivered on the U.S. mainland were similar to those for all women on the mainland. By contrast, among all 52,747 births in Puerto Rico in 2002, 45% were by cesarean delivery; among births in Puerto Rico to women without a previous cesarean delivery, 33% were primary cesarean deliveries (4). In addition, during 1996--2002, annual rates of vaginal births after cesarean delivery (VBAC) (i.e., per 100 live births to women who had a previous cesarean delivery) were lower in Puerto Rico than on the U.S. mainland. To compare trends in cesarean delivery during 1992--2002 among Puerto Rican women who delivered in Puerto Rico and on the U.S. mainland, CDC and the Puerto Rico Department of Health analyzed birth certificate data from the National Vital Statistics System (NVSS). This report summarizes the results of that analysis, which determined that, during 1992--2002, total and primary cesarean rates were consistently higher in Puerto Rico than among Puerto Rican women on the mainland. From 1996 to 2002, total and primary cesarean rates increased for Puerto Rican women in both places of delivery, but rates increased more sharply for women in Puerto Rico than on the mainland. The results suggest that measures to reduce the number of cesarean deliveries in Puerto Rico should focus on lowering the rate of primary cesarean deliveries, especially among women at low risk for a cesarean delivery.* NVSS birth certificates in Puerto Rico and on the U.S. mainland record data regarding method of delivery (i.e., vaginal, VBAC, primary cesarean, or repeat cesarean) (4). In Puerto Rico, during 1992--2002, approximately 82%--85% of birth certificates listed Puerto Rico as the birthplace of the mother, and 10%--13% listed the mother's birthplace as the U.S. mainland; approximately 5% of mothers who were born outside of Puerto Rico or outside of the U.S. mainland were excluded from this analysis. Puerto Rican women were defined as 1) mothers delivering in Puerto Rico who were born in Puerto Rico or on the U.S. mainland and 2) mothers delivering on the U.S. mainland who were residents of the mainland and reported their Hispanic origin as Puerto Rican on their infant's birth certificate. This analysis focused on differences by place of delivery (i.e., Puerto Rico versus the U.S. mainland). In addition to trends in cesarean rates during 1992--2002, certain maternal characteristics (e.g., age, level of education, and number of live births) were examined to determine any associations with rates of cesarean delivery and VBAC (5). Data also were analyzed to compare rates of cesarean delivery with the Healthy People 2010 objective (no. 16-9a) to lower the rate of cesarean deliveries to 15% among women at low risk for a cesarean delivery giving birth for the first time (6). Total and Primary Cesarean Deliveries and VBACsDuring 2002, Puerto Rican women had 50,553 live births in Puerto Rico. From 1992 (31.4%) to 1996 (31.7%), the annual total cesarean delivery rate in Puerto Rico remained stable before increasing by 42% from 1996 to 2002 (45.0%) (Figure 1). Primary cesarean delivery rates in Puerto Rico increased by 4% from 1992 (21.3%) to 1996 (22.1%), then increased by 52% from 1996 to 2002 (33.5%) (Figure 2). The VBAC rate in Puerto Rico remained stable at 8.1% during 1992--1996 before decreasing by 56% from 1996 to 2002 (3.6%) (Figure 2). During 2002, Puerto Rican women had 56,321 live births on the U.S. mainland. The annual total cesarean delivery rate for Puerto Rican women delivering on the mainland declined from 1992 (21.9%) to 1996 (20.8%), then increased by 26% from 1996 to 2002 (26.2%) (Figure 1). Primary cesarean delivery rates declined from 1992 (15.2%) to 1996 (14.6%), then increased by 24% from 1996 to 2002 (18.1%) (Figure 2). The VBAC rate for Puerto Rican women delivering on the mainland increased from 1992 (25.0%) to 1996 (31.2%), then decreased by 51% from 1996 to 2002 (15.2%) (Figure 2). Cesarean Delivery and Maternal CharacteristicsFrom 1992 to 2002, both in Puerto Rico and on the U.S. mainland, rates of total cesarean delivery for Puerto Rican women increased with maternal age and within age groups (Table). In Puerto Rico, the greatest increase was in the youngest group (aged <20 years), doubling from 18.5% to 37.6%. On the mainland, the greatest increase was among women aged 35--39 years, increasing 23% from 33.2% to 40.9%. During 2002, the highest rates both in Puerto Rico and on the mainland were for women aged >40 years (63.9% and 44.6%, respectively). Total cesarean delivery rates increased from 1992 to 2002 for women with one, two, and three or more live births (Table). In Puerto Rico, the largest increase (62%) was among women with three or more live births; however, the highest rate of cesarean delivery was for women delivering their second child (47.4%). On the U.S. mainland, the rate increased the most (24%) among women delivering their second child; these women also had the highest rate (27.2%) of cesarean delivery. In both 1992 and 2002, total cesarean delivery rates both in Puerto Rico and on the U.S. mainland increased with education. In 2002, rates for Puerto Rican women with >16 years of education were 51.4% in Puerto Rico and 34.9% on the mainland (Table). Among women with <8 years of education, the cesarean delivery rate in Puerto Rico doubled from 1992 (18.2%) to 2002 (36.4%) and increased by 26% (from 17.7% to 22.3%) on the mainland. The percentages of Puerto Rican women giving birth for the first time who were at low risk for a cesarean delivery were similar in Puerto Rico (16,462 [82%]) and on the U.S. mainland (14,309 [83%]). Annual rates of cesarean delivery among these women increased in Puerto Rico by 39% from 1992 (32.3%) to 2002 (44.8%). By contrast, rates for Puerto Rican women delivering on the mainland increased by 11% from 1992 (20.3%) to 2002 (22.6%). Reported by: R Varela-Flores, MD, H Vázquez-Rivera, MD, Puerto Rico Dept of Health. F Menacker, DrPH, Div of Vital Statistics, National Center for Health Statistics; Y Ahmed, MD, AM Grant, PhD, DJ Jamieson, MD, MK Whiteman, PhD, Div of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion; SL Farr, PhD, EIS Officer, CDC. Editorial Note:In Puerto Rico, annual rates of total and primary cesarean delivery were stable during 1992--1996 before increasing sharply from 1996 to 2002. Nearly half of all live births in Puerto Rico in 2002 were by cesarean delivery. Rates of cesarean delivery and primary cesarean delivery were 72% and 85% higher, respectively, among Puerto Rican women in Puerto Rico than on the U.S. mainland. From 1992 to 2002, the greatest increases in rates of cesarean delivery in Puerto Rico were among the youngest and least educated women; however, the highest rates remained among women aged >40 years and those with the highest levels of education. During 2002, the rate of cesarean delivery among women at low risk for a cesarean delivery giving birth for the first time in Puerto Rico was 44.8%, nearly three times the Healthy People 2010 target of 15% for women at low risk for a cesarean delivery and nearly double the 22.6% rate for Puerto Rican women at low risk for a cesarean delivery who delivered on the U.S. mainland. The cesarean rate (22%) for first births to all women at low risk for a cesarean delivery who delivered in the United States was similar to that for Puerto Rican women. Cesarean deliveries put women at greater risk for maternal morbidity (1,2) and can lengthen hospital stays and make rehospitalization more likely (2,3). During 2002, among women delivering in Puerto Rico with a previous cesarean delivery, approximately 96% had a repeat cesarean delivery. Whether VBAC or repeat cesarean delivery poses greater risk for a mother and infant is unresolved (7). According to the American College of Obstetricians and Gynecologists, most women with one previous cesarean delivery are candidates for VBAC. However, individual risk factors need to be considered; therefore, the ultimate decision regarding mode of delivery should rest with the patient and her provider (8). Measures to reduce the cesarean delivery rate in Puerto Rico should focus on lowering the rate of primary cesarean deliveries, especially among women at low risk for a cesarean delivery (9). The findings in this report are subject to at least three limitations. First, because Hispanic ethnicity of the mother is not recorded on birth certificates in Puerto Rico, a small number of live births in Puerto Rico included in the analysis might have been to women who were born in Puerto Rico or on the U.S. mainland but were not of Puerto Rican origin. Second, certain information that might influence differences in rates of cesarean delivery and VBAC (e.g., reason for cesarean delivery, type of hospital, or type of insurance coverage) is not currently collected on birth certificates. Finally, no distinction could be made between cesarean deliveries that were elective and those resulting from medical indications or conducted as emergency procedures. Why cesarean delivery rates in Puerto Rico are higher and increasing at a faster rate than those among Puerto Rican women delivering on the U.S. mainland is not known. High rates of cesarean delivery also have been reported among women delivering in certain Latin American countries, with rates highest in private hospitals (10). The higher rates in Puerto Rico might be associated with differences in maternal characteristics, attitudes toward cesarean delivery, obstetric practices, or health insurance coverage. Further research is needed to examine these factors and their potential association with rates of cesarean delivery and VBAC among Puerto Rican women. References
* A singleton pregnancy of >37 weeks' gestation with a vertex presentation (head facing downward in the birth canal). Based on Healthy People 2010 objective 16-9a for women giving birth for the first time with a singleton pregnancy.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 1/26/2006 |
|||||||||
|