|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
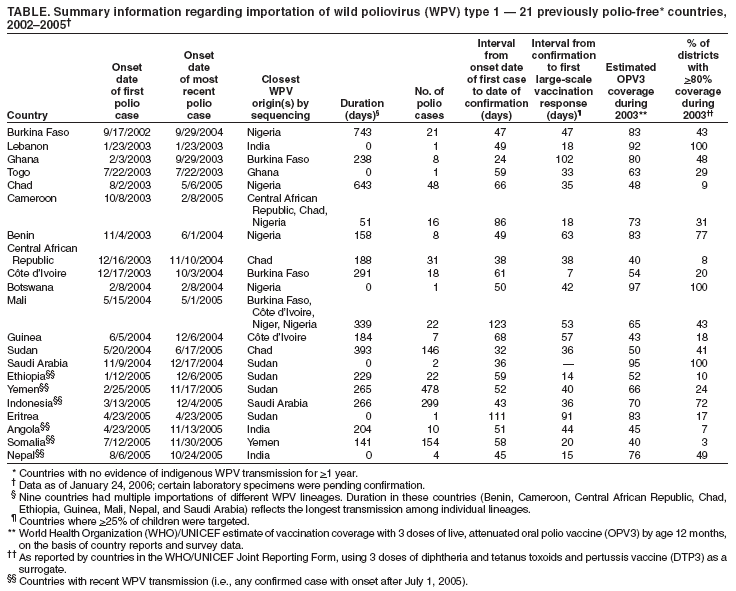
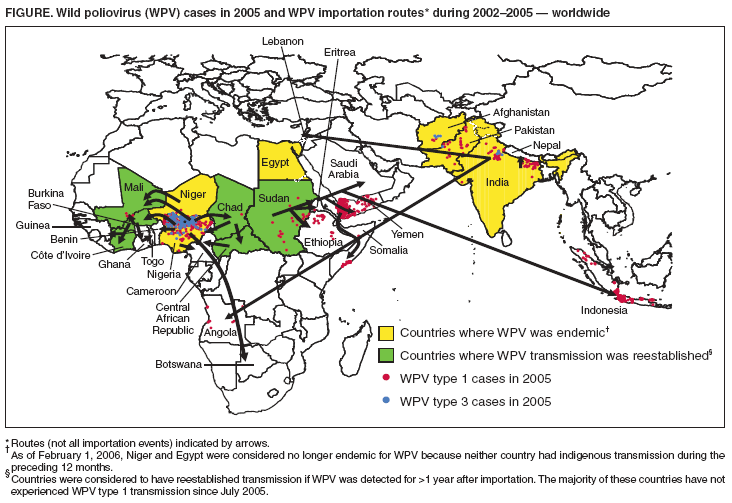
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Resurgence of Wild Poliovirus Type 1 Transmission and Consequences of Importation --- 21 Countries, 2002--2005After the 1988 World Health Assembly resolution to eradicate poliomyelitis globally,* the number of polio-endemic countries decreased from 125 in 1988 to six† (Afghanistan, Egypt, India, Niger, Nigeria, and Pakistan) in 2003 (1). However, during 2002--2005, a total of 21 previously polio-free countries§ were affected by importations of wild poliovirus (WPV) type 1 from the six remaining countries (primarily Nigeria) where WPV was endemic; four countries (Indonesia, Somalia, Sudan, and Yemen) had outbreaks of >100 polio cases (1,2).¶ By the end of 2005, WPV transmission in all 21 countries except Somalia had been interrupted or substantially curtailed. This report summarizes WPV importations into polio-free countries during 2002--2005 and the status of WPV transmission in these countries as of January 24, 2006, and describes actions that polio-free countries can take to improve importation preparedness. Origins and Timelines of ImportationsComprehensive sequencing data enable tracing of the origins and routes of virus importations.** Of 21 previously polio-free countries with importations since 2002, a total of 11 countries in Africa detected WPV type 1 during September 2002--June 2004; the virus was imported directly from Nigeria into Benin, Botswana, Burkina Faso, Cameroon, and Chad and indirectly from Nigeria through neighboring countries to Central African Republic, Côte d'Ivoire, Ghana, Guinea, Mali, and Togo (Figure). The number of reported polio cases resulting from a single importation ranged from one in multiple countries to 44 in Chad†† (Table). In addition, WPV type 1 of Nigerian origin was transmitted into seven other countries after virus from the Chad outbreak spread to Sudan in mid-2004. During November 2004--July 2005, WPV from Sudan spread to Eritrea, Ethiopia, Saudi Arabia, and Yemen; subsequently, WPV was imported into Indonesia from Saudi Arabia and into Somalia from Yemen. The number of polio cases ranged from one in Eritrea to large outbreaks in Yemen (478 cases), Indonesia (299), Somalia (154), and Sudan (146§§) (4--6). WPV type 1 originating from India has resulted in 15 polio cases in three countries since 2002. WPV type 1 was imported into Lebanon (one case in January 2003), Angola (10 cases during April--November 2005) (7), and Nepal (four cases during August--October 2005 from multiple importations) (Figure, Table). Consequences of WPV ImportationImported WPV did not result in sustained transmission in eight of the 21 countries, including four countries (Botswana, Eritrea, Lebanon, and Togo) with only one case and four countries (Benin, Cameroon, Nepal, and Saudi Arabia) with either polio cases not directly linked genetically or epidemiologically or with a duration of WPV transmission of <6 months. In the remaining 13 countries, imported WPV caused multiple-case outbreaks lasting >6 months. In eight (Burkina Faso, Central African Republic, Chad, Côte d'Ivoire, Ghana, Guinea, Mali, and Sudan) of the 13 countries, transmission is considered to have stopped,¶¶ with a median interval between the first and the last case of 315 days (range: 184--743 days). The eight countries without sustained WPV transmission differed in other ways from the 13 countries with sustained transmission. According to World Health Organization (WHO)/UNICEF estimates for 2003, the eight countries had median vaccination coverage (3 doses of live, attenuated oral polio vaccine [OPV3] by age 12 months) of 83% compared with a median coverage of 52% in the other 13 countries (p = 0.001, Wilcoxon rank-sum test). The median proportion of districts with reported coverage of at least 80% also differed: 63% for the eight countries without sustained WPV transmission and 20% for the 13 countries with sustained transmission (p = 0.009) (8). Timeliness of Detection and ResponseThe median interval from onset of paralysis in the first case to laboratory confirmation of WPV was 51 days (range: 24--123 days) in the 21 countries with importations (Table). The median interval from laboratory confirmation to supplementary immunization activity (SIA)*** was 37 days (range: 7--102 days). All countries conducted multiple SIA rounds (mean: four rounds; range: two to 10 rounds) in response to WPV importations, some of which had already been planned because of the known high risk for importations. SIAs in west and central Africa and Sudan were synchronized among as many as 22 countries. The median interval from onset of the first case to the first large-scale (i.e., >25% of children) vaccination response was 92 days (range: 60--202 days). Countries with Ongoing TransmissionIn six countries (i.e., five with sustained transmission [Angola, Ethiopia, Indonesia, Somalia, and Yemen] plus Nepal with repeated importations), transmission was detected during the most recent 6-month period. Nepal reported a case with onset on October 24, 2005, and ongoing transmission, although unlikely, cannot be excluded. The following are summaries of the status in the three countries with recent WPV transmission and large outbreaks. Yemen. Six years after its last clinically confirmed polio case in 1999 and 4 years after conducting its last national immunization day (NID) in 2002, Yemen confirmed its first case of imported WPV infection (onset February 2005) in late April 2005. Even before the first case in the outbreak was identified, an NID round was conducted in mid-April 2005 in response to the threat of importation from Sudan. Six additional NIDs were conducted during May--December 2005, with type 1 monovalent OPV (mOPV1†††) used for three of the six rounds. A total of 478 polio cases have been reported from 21 of 22 governorates, with only five cases reported after the September NID; the most recent onset was November 17, 2005. Indonesia. Ten years after its last clinically confirmed polio case and 2.5 years after its most recent SIA, Indonesia confirmed its first case of imported WPV infection (onset in March 2005) in West Java Province in May 2005. By the time the first response SIA was conducted, targeting 6.4 million children aged <5 years in three provinces of the island of Java (25% of the national target population), 99 additional cases had occurred; the outbreak had grown to 252 cases in seven provinces when the first of three full NIDs targeting 24 million children was conducted in August 2005. To date, 299 cases have been reported from 10 provinces on Java and Sumatra; 11 cases have been reported since the September NID campaign, with the most recent onset on December 4, 2005. Somalia. The first case of polio in Somalia in 2005, which resulted from importation of WPV from Yemen, had onset of paralysis in the capital city of Mogadishu in July 2005 and was confirmed in September 2005. Before this case occurred, the last confirmed polio case in Somalia (WPV type 3) occurred in October 2002. Because of the difficulties of implementing polio eradication strategies in Somalia, which has been affected by chronic conflict and security problems, OPV SIA campaigns have been conducted in Somalia every year. Four NIDs (two using mOPV1) were conducted during February--July 2005 in response to the risk for WPV importation from nearby countries. After the onset of polio cases in July, three additional NID rounds were conducted during August--November 2005. To date, 154 cases have been confirmed, with the most recent onset on November 30, 2005; the cases have included 140 from Mogadishu, 11 from an adjacent district, one from a district west of Mogadishu, and two from a district in northwest Somalia near the Ethiopian border. Reported by: Polio Eradication Initiative; Global Polio Laboratory Network, World Health Organization, Geneva, Switzerland. Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Global Immunization Div, National Immunization Program, CDC. Editorial Note:Strategies for achieving polio eradication include high routine vaccination coverage, high-quality SIAs, and acute flaccid paralysis (AFP) surveillance that meets WHO performance indicators. Cessation of SIAs in portions of northern Nigeria during 2003--2004 (2) and the ongoing deficiencies in vaccinating children through routine services in many countries resulted in regional spread of WPV type 1 from Nigeria into previously polio-free countries, followed by intercontinental spread to the Middle East and Asia. Continuing transmission in northern India similarly resulted in intercontinental spread of WPV type 1 to Lebanon and Angola and contiguous spread to Nepal. During 2005, WPV type 3 polio cases were limited to five countries (Afghanistan, India, Niger, Nigeria, and Pakistan). WPV type 3 typically is more geographically localized than WPV type 1 and is less commonly associated with importation events or subsequent outbreaks. WPV type 1 importations and subsequent transmission has had a major impact (e.g., on finances and human resources) on the Global Polio Eradication Initiative. During 2005, a total of 1,000 polio cases (54% of the global total of 1,856) were reported from countries with outbreaks caused by importation, more than from the six remaining polio-endemic countries. Most outbreaks required multiple rounds of large-scale SIAs to control and stop transmission. Countries and international polio partners had to urgently secure additional financing and vaccine. Because of these efforts, transmission of WPV after importation has been halted or curtailed in all countries experiencing importations since 2002, except Somalia. The relative ease with which WPV type 1 originating from Nigeria spread through west and central Africa to the Horn of Africa, the Arabian Peninsula, and Indonesia, underscores the immunity gaps among children in the affected countries. In the 13 countries experiencing outbreaks after importation, routine immunization programs remained weak, and immunity gaps at the subnational level enabled sustained transmission of WPV. The majority of countries had discontinued large-scale SIAs soon after becoming polio-free because of funding limitations. Inability to achieve or maintain high routine vaccination coverage in the absence of periodic NIDs made some countries with imported WPV vulnerable to reestablishment of WPV transmission within their borders. When periodic SIAs are conducted, planning and supervised implementation to ensure campaign quality and effectiveness are critical. Delay in effective response vaccination contributes to extended duration of WPV transmission, which facilitates further global spread. Although surveillance systems detected and confirmed initial imported cases within the recommended 60-day period in the majority of countries, response vaccination often was not implemented within the recommended 28-day interval after WPV confirmation. Only six (30%) of 20 countries met this target. WPV importations from polio-endemic countries into polio-free areas will continue to occur until endemic transmission is interrupted globally. The risk for importation is greatest for countries adjacent to polio-endemic countries; however, globalization and international migration pose a risk for reintroduction of WPV to all countries. Maintaining polio eradication strategies and preparedness can prevent WPV spread subsequent to importation. All polio-free countries are advised to maintain sensitive, efficient AFP surveillance systems in all areas to detect importations rapidly and to maintain sufficient levels of immunity against polioviruses through routine immunization programs or, where necessary, SIAs. Countries should prepare and maintain plans for timely, large-scale, high-quality response SIAs in case importation occurs. WHO's Advisory Committee on Polio Eradication recommends that any polio-free country that detects imported WPV take the following measures immediately: 1) obtain a risk assessment from an international expert group and prepare a large-scale vaccination response plan within 72 hours of case confirmation; 2) conduct at least three large-scale, house-to-house immunization campaigns using type-specific mOPV, initiating the first round within 28 days of case confirmation§§§; 3) target a large number (e.g., at least 2--5 million) of children aged <5 years in the affected and adjacent geographic areas; and 4) initiate independent SIA monitoring to ensure adequate coverage, with rounds repeated in areas with <90% vaccination coverage (10). Adherence to these recommendations and timelines, in combination with enhanced surveillance and investigation, can minimize the impact of WPV importation and facilitate global eradication of polio. Despite substantial progress toward polio eradication during 2002--2005, the potential for WPV importation and transmission underscores the importance of sustained political and financial support to avoid resurgence of polio worldwide. References
* World Health Assembly. Global eradication of poliomyelitis by the year 2000: resolution of the 41st World Health Assembly. Geneva, Switzerland: World Health Organization; 1988 (WHA resolution no. 41.28). † As of February 1, 2006, Niger and Egypt were considered no longer endemic for WPV because neither country had indigenous transmission during the preceding 12 months. § Countries with no evidence of indigenous WPV transmission for >1 year. ¶ In this report, Niger was not included among the 21 polio-free countries with imported WPV because Niger was not considered polio-free at the beginning of 2005. ** The sequence of the complete VP1 coding region is determined by using automated cycle-sequencing procedures described previously (3) and by comparing the resulting sequences with those in a database of all recent poliovirus isolates. The origins and routes of virus importation are then derived from phylogenetic analysis. †† Imported virus resulted in 48 cases from three importations in Chad; transmission of older endemic lineages of WPV type 3 accounted for two cases. §§ Imported virus resulted in 146 cases in Sudan; transmission of nonimported endemic lineages of WPV type 1 accounted for five other cases and WPV type 3 for three cases. ¶¶ For the purposes of this analysis, transmission after importation of WPV type 1 was considered to have stopped if countries did not detect WPV during the preceding 6 months. *** SIAs consist of 1) national immunization days (NIDs), nationwide mass campaigns conducted during a short period (i.e., days to weeks) during which a dose of OPV is administered to all children (usually aged <5 years) regardless of previous vaccination history; 2) sub-NIDs (SNIDs), which are campaigns similar to NIDs but confined to certain parts of the country; or 3) mopping-up intensive focal campaigns focusing on high-risk areas after poliovirus isolation in countries that are endemic for WPV. ††† mOPV1 has greater immunogenicity for WPV type 1 per dose than trivalent OPV (9). §§§ Continuing with at least two NID rounds after the last virus is detected.
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 2/16/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|