 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Illness Surveillance and Rapid Needs Assessment Among Hurricane Katrina Evacuees --- Colorado, September 1--23, 2005After Hurricane Katrina struck the U.S. Gulf Coast on August 29, 2005, approximately 200,000 evacuees were sent to shelters in 18 states (1). On September 3, 2005, Colorado was asked to assist in sheltering some of the evacuees; the next day the first evacuees were airlifted into the Denver area, where they were housed at the former Lowry Air Force Base. During the next 4 weeks, 3,600 evacuees registered at Lowry, with an average of 400 persons in residence per day. Other persons self-evacuated to other parts of the state, including approximately 2,000 who went to Colorado Springs. In all, an estimated 6,000 evacuees were living throughout Colorado in the weeks after Hurricane Katrina. As a result of the influx of evacuees, the Colorado Department of Public Health and Environment (CDPHE) and the Tri-County Health Department (TCHD) established surveillance systems to provide early detection of outbreaks and determine the scope of medical conditions of evacuees. A rapid needs assessment also was conducted at the local level to assess acute medical and other needs of evacuees. Results indicated that many evacuees had chronic conditions and approximately half planned to remain in the area, suggesting a long-term need for increased health-related and other services. In addition, the most common acute symptoms were related to altitude sickness, requiring education of incoming Gulf Coast evacuees regarding the effects of the mile-high altitude in Denver. Local and State SurveillanceAs evacuees arrived at the Lowry site during the week of September 4, 2005, TCHD established syndromic surveillance at the Lowry medical clinic, an outpatient facility. Beginning September 7, the clinic reported various syndromes or types of symptoms among evacuees. Gastrointestinal (i.e., vomiting or diarrhea), respiratory (i.e., acute cough and fever), and dermatologic symptoms (i.e., rash with fever) were assessed, along with certain chronic disease--related syndromes (e.g., acute chest pain, stroke, or psychiatric illnesses). Report forms were faxed daily to TCHD, which monitored the information for baseline illness rates and potential outbreaks. Local surveillance was conducted during September 7--September 21, when 509 evacuee visits were made to the Lowry clinic. The number of daily visits declined from 83 to 16, as evacuees moved out of Lowry and into the surrounding community. During the surveillance period, 10 cases of vomiting or diarrhea were identified, along with 10 cases of acute cough and fever and 15 cases of wound infection or cellulitis; 17 visits were related to mental health. The majority of visits were for medication refills, according to the head clinician at the Lowry clinic. These visits were not counted by TCHD. No outbreaks of infectious disease were identified. On September 9, 2005, CDPHE implemented statewide surveillance of hospital emergency department (ED) visits among evacuees. A Colorado Health Alert Network (HAN) message to EDs requested that they identify evacuee visits and inform their hospital infection-control practitioner (ICP). A separate HAN message to ICPs requested that they report these visits through their usual disease-reporting process and that they report retroactively to September 1. Surveillance was continued through September 23. During September 1--23, a total of 124 visits were reported by Colorado hospital EDs in 10 counties. ED visits were reported from 17 hospitals, although four Denver-area hospitals and one Colorado Springs hospital accounted for 75% of reports. Among the evacuees who visited EDs, 74 (59.7%) were female; 12 (9.7%) were aged <19 years, 34 (27.4%) were aged 20--39 years, 46 (37.1%) were aged 40--64 years, and 32 (25.8%) were aged >65 years. The most common reasons for ED visits included pain or headache (20.1%), other reason (e.g., dizziness, allergic reaction, or sore throat) (15.3%), medication refill (12.9%), chronic disease (10.5%), and respiratory illness (10.5%) (Table 1). Twenty-eight persons (22.5%) were admitted to a hospital; one person died suddenly at a Lowry dormitory after being evaluated in a nearby ED and refusing hospital admission for pneumonia. Rapid Needs AssessmentDuring September 4--9, 2005, TCHD conducted a rapid needs assessment of a sample of newly arriving evacuees at Lowry. All evacuees who registered during the first week at Lowry were sent by bus to an American Red Cross family assistance center to register with the Federal Emergency Management Association. Among eight buses arriving from Lowry, two were selected at random. Heads of all 106 households with members on the two buses were interviewed; all agreed to participate. Among heads of households surveyed, 55% were non-Hispanic blacks, 36% were non-Hispanic whites, and 6% were Hispanic whites. The number of family members per household ranged from one to 30 (an extended family living in a mobile home with some members sleeping outside); the median was 2.0, and the mean was 3.8. The most common acute medical conditions among households reporting one or more conditions were related to altitude sickness (e.g., dehydration, lightheadedness, or problems breathing) (Table 2). Common chronic medical conditions included hypertension (28.4%), depression or other psychiatric illness (23.2%), asthma or chronic lung disease (21.1%), cardiovascular disease (17.9%), and diabetes (13.7%). Among households surveyed, 60.2% had one or more family members requiring prescription medications. Of those households requiring prescription medications, 38.8% were lacking them at the time of the survey, and 42.7% had gone without medications at some point as a result of Hurricane Katrina. The most common long-term service needs included medical services, health insurance, housing assistance, and clothing (particularly winter clothing) (Table 3). Although the majority of services already were being offered, many evacuees seemed unaware of their availability. Among households surveyed, 49.1% of evacuees reported planning to stay in Colorado permanently, suggesting the need to provide these services over an extended period. As a result of this assessment, several recommendations were made to meet the needs of evacuees arriving in subsequent weeks. TCHD nurses provided altitude sickness education to all evacuees during their initial registration at Lowry, and evacuees were advised of the available services. In addition, other agencies, including CDPHE and the American Red Cross, were provided summaries of the needs assessment to better meet the long-term needs of evacuees. Reported by: L Dippold, MPH, JL Patnaik, MHS, RL Vogt, MD, Tri-County Health Department, Greenwood Village; K Gershman, MD, S Burnite, Colorado Dept of Public Health and Environment. T Ghosh, MD, W Bamberg, MD, EIS officers, CDC. Editorial Note:In post-disaster situations, timely surveillance systems and rapid needs assessments are needed to provide information regarding outbreaks, disaster-related morbidity and mortality, and medical and nonmedical needs that can guide public health responses (2--5). These activities are needed not only in the immediate disaster area, but also in outside areas that house displaced persons (6,7). Both surveillance systems described in this report were implemented within 1 week of the arrival of evacuees, enabling timely surveillance. Although no outbreaks of infectious disease were detected, surveillance efforts provided information regarding the scope of medical issues affecting evacuees, which was useful in planning for ongoing medical needs. The rapid needs assessment, which also was completed within 1 week of the arrival of evacuees, provided insight into their medication, chronic disease, and mental health needs. Meeting these needs was important to avoid the long-term complications of chronic disease and mental health conditions among the 49.1% of evacuees who indicated they planned to remain in the area. The assessment also helped to identify a need for altitude sickness education. The findings in this report are subject to at least two limitations. First, illness surveillance was limited to patients who visited EDs and therefore did not include results from persons who sought treatment at outpatient health-care clinics. Second, the rapid needs assessment was conducted during a 1-week period and considered only the immediate needs of newly arriving evacuees; those needs might have changed over time. The state-level ED surveillance system demonstrated the ability to rapidly adapt an existing disease reporting system to accommodate a short-term surveillance need and provide information regarding potential outbreaks of infectious disease. Rapid needs assessments such as the one described in this report should be conducted routinely after a natural disaster, both at the immediate disaster site and in evacuation areas, because needs can vary by location (7). Data from surveillance and assessment activities can be used to direct immediate assistance to evacuees and guide program planning that will adequately provide for long-term evacuee needs. Acknowledgments The findings in the report are based, in part, on contributions by S Weinberg, L Smith, and J Uhernik, Tri-County Health Dept, Greenwood Village; members of the El Paso County Dept of Health and Environment, Colorado Springs; and N Enyart, L Loveland, and A Cronquist, Colorado Dept of Public Health and Environment. References
Table 1 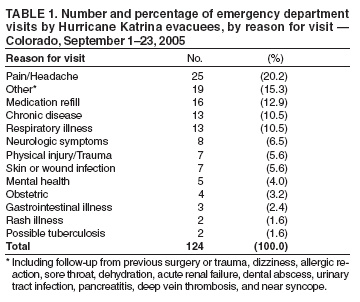 Return to top. Table 2 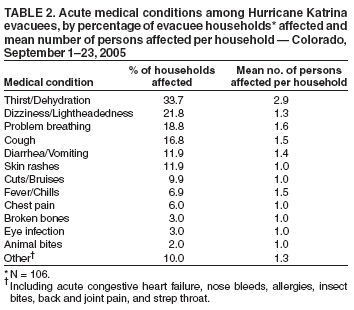 Return to top. Table 3 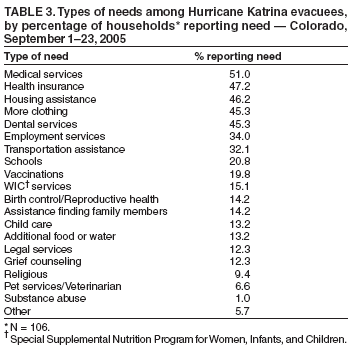 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 3/9/2006 |
|||||||||
|