|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
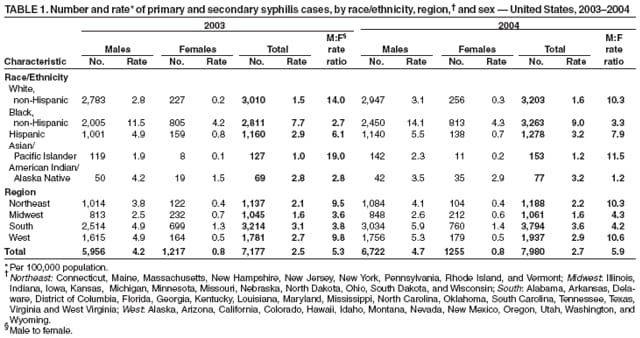
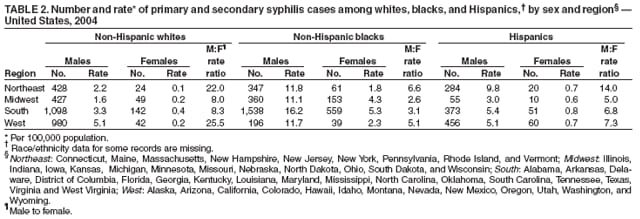
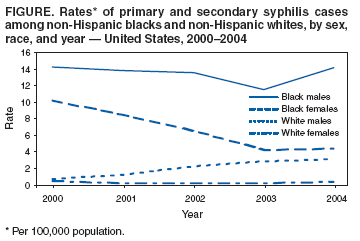
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Primary and Secondary Syphilis --- United States, 2003--2004In 2000, the rate of primary and secondary (P&S) syphilis in the United States was 2.1 cases per 100,000 population, the lowest since reporting began in 1941. From 2001 to 2004, the P&S syphilis rate increased to 2.7, primarily as a result of increases in cases among men who have sex with men (MSM). To characterize the recent epidemiology of syphilis in the United States, CDC analyzed national notifiable disease surveillance data for 2000--2004, focusing on 2003--2004.* This report describes the results of that analysis, which indicated that the disparity between syphilis rates among blacks and whites† in 2004 increased for the first time since 1993 and is associated with a substantial increase of syphilis among black men. Syphilis rates continue to increase among MSM. After declining for 13 years, the rate of P&S syphilis in 2004, compared with 2003, increased in the South§ and remained the same among women. The findings underscore the need for enhanced prevention measures among blacks and MSM. In addition, enhanced surveillance is needed to detect any early increases in P&S syphilis among women. CDC analyzed surveillance data reported weekly from health departments nationwide during 2000--2004. Data included patient demographics (i.e., age, sex, race/ethnicity, and county of residence) and stage of syphilis. Data on P&S syphilis were analyzed because these cases represent incidence (i.e., newly acquired infections within the specified period). P&S syphilis rates were calculated using population denominators from the U.S. Census Bureau (1). Because states do not routinely report information on sexual practices or sex of sex partners, male-to-female (M:F) rate ratios were used as a surrogate measure to monitor occurrence of syphilis among MSM and were calculated by dividing the male case rate by the female case rate for a specified period. M:F rate ratios in excess of 1:1 suggest male-to-male transmission. From 2000 to 2004, the number of cases of P&S syphilis increased from 5,979 to 7,980, and the rate increased from 2.1 to 2.7 cases per 100,000 population. Of the 7,980 cases of P&S syphilis reported in 2004, approximately 84% (6,722) occurred among men. The rate of P&S syphilis among men increased from 2.6 to 4.7. Among women, the rate of P&S syphilis decreased from 1.7 to 0.8 from 2000 to 2003 and remained at 0.8 in 2004, the first time since 1991 that the rate among women did not decrease. The M:F rate ratio increased steadily from 1.5 in 2000 to 5.3 in 2003, but the increase slowed in 2004 (M:F rate ratio: 5.9; 11% increase from 2003). P&S syphilis incidence varied by race/ethnicity. From 2000 to 2003, the incidence among blacks decreased from 12 to 7.7 cases per 100,000 population but increased to 9.0 in 2004. Rates increased among whites each year from 2000 to 2004 (from 0.5 to 1.6), Hispanics (from 1.6 to 3.2), and Asian/Pacific Islanders (from 0.3 to 1.2). The rate among American Indian/Alaska Natives increased from 2000 to 2001 (from 2.2 to 3.8), decreased to 2.1 in 2002, and then increased to 3.2 in 2004. Although the rate of P&S syphilis among blacks increased in 2004, substantial increases occurred only among black men (14 cases per 100,000 population in 2004 versus 12 in 2003). For the first time since 1991, rates among black women did not decrease (4.3 in 2004 versus 4.2 in 2003). From 2000 to 2004, the black M:F rate ratio increased from 1.4 to 3.3. Racial/ethnic disparities in P&S syphilis persist. The increase in the overall P&S rate among blacks in 2004 represents the first year since 1993 that the disparity between black and white rates of P&S syphilis increased. In 2003, the rate among blacks was 5.1 times that among whites (7.7 versus 1.5 cases per 100,000 population). In 2004, the rate among blacks increased and was 5.6 times higher than that among whites (9.0 versus 1.6). From 2000 to 2004, rates of P&S syphilis were higher among black men and women than among white men and women, respectively (Figure). Rates among black men increased by 23% from 2003 to 2004, whereas rates among black women increased by 2% (Table 1). Among Hispanics, the rate among men increased by 12% and decreased among women by 13%. During 2000--2004, although the M:F rate ratio among whites was higher each year than for blacks and Hispanics, from 2003 to 2004, this ratio decreased among whites (from 14 to 10) and increased among blacks (from 2.7 to 3.3) and Hispanics (from 6.1 to 7.9) (Table 1). By region, rate increases from 2003 to 2004 were highest in the South (3.1 versus 3.6 cases per 100,000 population; 16% increase), followed by the West (2.7 versus 2.9; 7.4% increase), and the Northeast (2.1 versus 2.2; 4.8% increase) (Table 1). For the Midwest, rates remained constant at 1.6. The rate increase in the South represents the first time since 1991 that rates of P&S syphilis increased in that region. In 2004, rates of P&S syphilis varied within regions of the United States by race/ethnicity and sex (Table 2). In each region, P&S syphilis rates among black men and women exceeded those of whites and Hispanics. Reported by: JF Beltrami, MD, HS Weinstock, MD, SM Berman, MD, EB Swint, MS, KA Fenton, MD, Div of Sexually Transmitted Disease Prevention, National Center for HIV, STD, and TB Prevention; HA Lindstrom, PhD, EIS Officer, CDC. Editorial Note:From 2000 to 2004, rates of P&S syphilis increased among men and were higher among blacks and Hispanics than among whites. The rate of P&S syphilis among blacks was 5.1 times higher than whites in 2003, but 5.6 times higher in 2004. This represents the first increase in the disparity between black and white rates since 1993. The increasing M:F rate ratio suggests that increases are still occurring among MSM. CDC has estimated that in 2004, approximately 64% of all P&S syphilis cases were among MSM.¶ After 13 years of decline, rates of P&S syphilis in 2004 increased in the South and did not decrease among women. The national Syphilis Elimination Effort (SEE) began in 1999 (2) and focused primarily on heterosexual blacks living in the South. The findings described in this report indicate that prevention measures for MSM of all races/ethnicities should be strengthened throughout the United States. Moreover, gains already achieved in reducing heterosexual and congenital syphilis must be maintained to reach national health objectives to reduce P&S syphilis among women (1). The SEE program is assessing its activities and modifying its strategies for addressing the changing epidemiology of syphilis in the United States. Reported increases in incidence of P&S syphilis among MSM have been characterized by high rates of human immunodeficiency virus (HIV) co-infection, high-risk sexual behavior, and use of drugs such as methamphetamines (3). Syphilis increases have occurred among MSM who have met sex partners in Internet chat rooms (4). As a result, local program staff are encouraged to consider the effect of the Internet on syphilis and HIV epidemiology and to explore the use of the Internet as a tool in the prevention of sexually transmitted diseases (STDs). Internet-based STD prevention and control activities have been used to reach high-risk MSM populations (5). Infected non--gay-identified (NGI) MSM who also have female partners likely contribute to P&S syphilis among women (6). Targeting STD-prevention messages to high-risk NGI MSM remains a challenge, particularly among men in racial/ethnic minority populations. Suggested strategies for reaching this population include outreach through partnerships with community-based organizations already working within NGI MSM communities and Internet-based health information dissemination (7). Public health STD programs should strengthen existing collaborations with private health-care providers and initiate new ones. A national survey revealed that many physicians fail to report STD cases to local health departments, despite being mandated to do so, and that physicians rely on patients to notify their partners of their STD diagnosis, a strategy with unknown efficacy for STD treatment (8). Increasing provider awareness of P&S syphilis among MSM has been demonstrated to increase case reporting (9), which is essential to successful partner notification and treatment activities implemented by local health departments. Concerns regarding the anonymity of sex partners of MSM and men's willingness to cooperate with health department staff for purposes of partner identification pose challenges to traditional partner-notification strategies (10). Health departments that cooperate with other community and health-care organizations and place partner notification in the context of the broader health-care needs of MSM have been more successful in notifying the partners of MSM infected with syphilis (9). The findings in this report are subject to at least three limitations. First, syphilis case-report data likely underestimate the true burden of disease in the United States because of underreporting, infected persons not accessing health-care, and persons who are not screened. Therefore, these data should be interpreted with caution. Second, analyses by race/ethnicity are limited by the small number of Asian/Pacific Islanders and American Indian/Alaska Natives reported with P&S syphilis. Finally, data on the sex of sex partners were not available. In 2005, CDC requested that standardized data on the sex of sex partners be collected and submitted to CDC with the surveillance data already reported weekly from health departments nationwide. In addition, a new syphilis interview record is being developed to capture information about the sex of sex partners and other key risk factors. In the interim, high M:F rate ratios are used as a surrogate measure for MSM transmission. Despite successes in decreasing the overall rate of P&S syphilis in the United States, challenges remain, particularly the need to improve the detection and prevention of syphilis among women and MSM. Rates among men continue to increase, and the decrease in rates among women that began in 1991 ended in 2004. Public health practitioners should consider the use of Internet-based strategies for health information dissemination and partner notification, realizing the challenge of locating sex partners about whom limited information is known (4,5). Nevertheless, public health practitioners should consider the use of Internet-based strategies for health information dissemination and partner notification. Reported use of methamphetamine is an added concern (3). Local health departments and SEE should focus on expanding public and private partnerships to improve case identification and reporting, partner-notification programs, and outreach to NGI MSM. Acknowledgment The findings in this report are based, in part, on contributions by state and local health departments. References
* Data for 2003 are summarized for the reporting year December 29, 2002, through January 3, 2004. Data for 2004 are summarized for the reporting year January 4, 2004, through January 1, 2005. † For this report, persons identified as white, black, Asian/Pacific Islander, American Indian/Alaska Native, and of other/unknown race are all non-Hispanic. Persons identified as Hispanic might be of any race. § Northeast: Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont; Midwest: Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin; South: Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia and West Virginia; West: Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming. ¶ Method of estimation presented at the Infectious Diseases Society of America 43rd Annual Meeting, San Francisco, CA, October 8, 2005 (Poster #906).
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 3/16/2006 |
|||||||||
|