|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
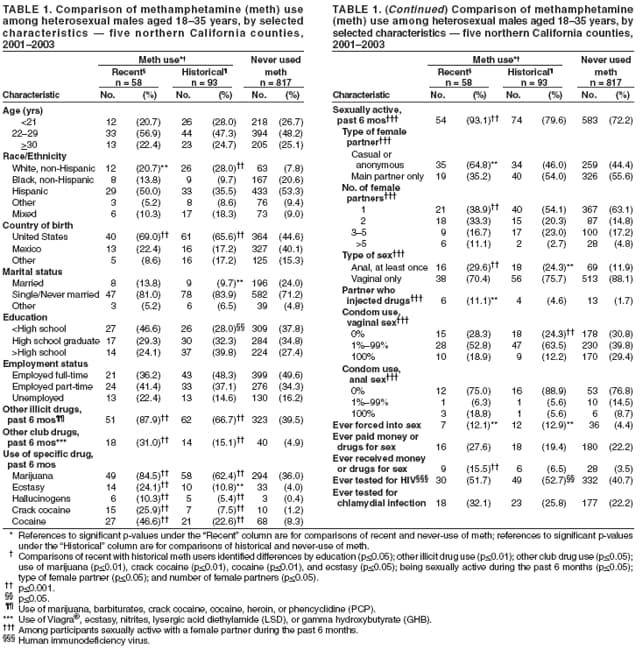
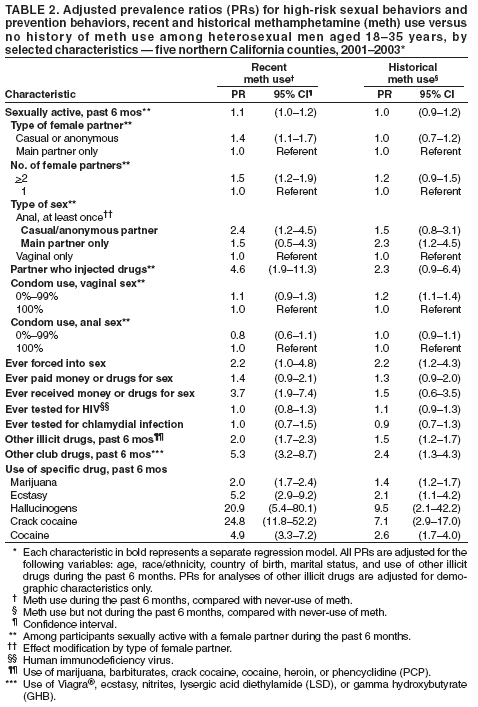
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Methamphetamine Use and HIV Risk Behaviors Among Heterosexual Men --- Preliminary Results from Five Northern California Counties, December 2001--November 2003Methamphetamine (meth) is a highly addictive stimulant that gained widespread popularity in California in the 1980s and has since spread to most regions of the United States, including rural areas (1). Analyses of survey data among noninjection-drug users from California in the mid-1990s determined that, among heterosexual persons and among men who had sex with men (MSM), meth users reported more sex partners, were less likely to report condom use, and were more likely to report sex in exchange for money or drugs, sex with an injection-drug user, and history of a sexually transmitted disease (STD) (2). Subsequent studies among MSM have indicated an association between meth use and sexual risk behaviors, syphilis infection, and incidence of human immunodeficiency virus (HIV) infection (3--5). Subsequent studies among heterosexual populations (6) have been less extensive than those among MSM and often have not used population-based samples nor adjusted for possible confounders. To further assess the association between meth use and high-risk sexual behaviors among heterosexual men, the California Department of Health Services, Office of AIDS, analyzed population-based data from five northern California counties in the HEY-Man (Health Evaluation in Young Men) Study. This report summarizes the results of that analysis, which determined that recent meth use was associated with high-risk sexual behaviors, including sex with a casual or anonymous female partner, anal intercourse, and sex with an injection-drug user. The results suggest the need for states to consider including referrals to meth prevention and treatment programs in their HIV prevention programs and for broader assessment of the relation between meth use and high-risk sexual behaviors. HEY-Man is a population-based, cross-sectional evaluation of HIV infection, STDs, and associated risk behaviors among men aged 18--35 years residing in low-income neighborhoods of Alameda, Contra Costa, San Francisco, San Joaquin, and San Mateo counties in northern California. The study protocol was approved by the institutional review boards of the State of California Health and Welfare Agency and the University of California, San Francisco. Within the five counties, low-income neighborhoods were defined as census block groups with median household incomes below the 10th percentile on the basis of data from the 2000 U.S. Census. City blocks were randomly sampled, without replacement, from these census-defined block groups. Trained field staff enumerated dwelling places in each sampled city block, then went door-to-door to locate male residents and request their participation. Repeat visits, including visits during evening hours and weekends, were made as necessary to identify all eligible men and request their participation. During December 2001--November 2003, the period for which data were available, 2,132 men were contacted; 1,692 (79%) were determined eligible (i.e., aged 18--35 years and residing in the selected neighborhoods), and 1,068 (63%) of those agreed to participate and were enrolled. A total of 1,011 participants completed a staff-administered interview conducted in English or Spanish. The study is scheduled for completion in June 2006. The HEY-Man questionnaire included a sexual-activity matrix in which field staff recorded the first name, nickname, initials, or alias of up to 10 persons with whom participants said they had vaginal or anal sex during the preceding 6 months. Questions were asked to determine the sex and category (i.e., main, casual, or anonymous) of each sex partner and whether acts included vaginal or anal intercourse with the partner. For this report, analyses were restricted to men who reported having female sex partners exclusively during the preceding 6 months; 43 men (4.1%) who reported having one or more male sex partners during the preceding 6 months were excluded, leaving 968 participants. Frequency of condom use was derived from the study's matrix as the sum of reported acts of vaginal and anal intercourse during which condoms were used, divided by the total number of acts of vaginal and anal intercourse. Meth use was divided into two categories: recent use (any use during the preceding 6 months) and historical use (use but not during the preceding 6 months). Participants also were asked if they had ever been tested for HIV or chlamydial infection and if they had ever given or received money or drugs for sex or been forced into sex by another male or female. Chi-square tests were conducted to compare the characteristics of participants (i.e., recent versus no reported meth use, historical versus no reported meth use, and recent versus historical meth use). Separate regression models were used to examine associations between meth use (independent variable) and dichotomously categorized sexual risk and protective behaviors. Regression models were adjusted for demographic characteristics that were significantly associated with recent or historical meth use and use of any other illicit drugs. Prevalence ratios and 95% confidence intervals were calculated using regression procedures for binomially distributed variables (7). Among the 968 participants, a larger percentage were non-white (Hispanic [51.1%] or non-Hispanic black [19.0%]), born in the United States (48.0%) or in Mexico (36.8%), single/never married (73.0%), and employed full- (47.8%) or part-time (34.4%). Meth use was reported among 151 (15.6%) participants, including 93 (9.6%) who reported historical use and 58 (6.0%) who reported recent use. The prevalence of recent meth use was higher among participants who were non-Hispanic white (11.9%), born in the United States (8.6%), single/never married (6.6%), and employed part-time (7.2%) or unemployed (8.3%). A greater percentage of recent meth users (93.1%) than men who reported never using meth (72.2%) had been sexually active with a female partner during the preceding 6 months (p<0.001) (Table 1). A greater percentage of meth users reported having anal sex with a female during this period than never users (recent users [29.6%; p<0.001] and historical users [24.3%; p<0.01] versus never users [11.9%]). Statistically significant differences with respect to other high-risk sexual behaviors were observed between recent meth users and never users. These differences included having a casual or anonymous female sex partner (recent users [64.8%] versus never users [44.4%]; p<0.01), having multiple partners (56.9% versus 26.3%; p<0.001), having a partner who injected drugs (11.1% versus 1.7%; p<0.01) during the preceding 6 months, and ever having received drugs or money for sex with a male or female partner (15.5% versus 3.5%; p<0.001). Regression analyses determined that recent meth users were more likely than men who had never used meth to be sexually active with a female partner, have multiple female partners, have a casual or anonymous female partner, have anal intercourse with a casual or anonymous female partner, have a female partner who injected drugs, or have ever received money or drugs for sex from a male or female partner (Table 2). Recent meth use was not associated with reported condom use during the preceding 6 months, but this might reflect overall infrequent condom use among the 968 men in the study population, who had a median of 48 reported acts of vaginal intercourse and a median of five uses of condoms during vaginal intercourse. Recent meth users were no more likely to have been tested for HIV or chlamydial infection than were men who had never used meth. Among historical meth users, sexual activity with higher HIV-transmission risk (i.e., anal sex) was identified primarily among those with main female sex partners only. Both recent and historical meth users were more likely to report they had ever been forced into sex by a male or female than men who had never used meth. After adjustment for demographic characteristics, recent and historical meth use was associated with recent use of one or more other illicit drugs,* use of club drugs,† and specific use of marijuana, ecstasy, hallucinogens (e.g., LSD), crack cocaine, and cocaine (Table 2). Reported by: CS Krawczyk, PhD, F Molitor, PhD, J Ruiz, MD, DrPH, M Facer, PhD, Office of AIDS, California Dept of Health Svcs; B Allen, MD, B Green-Ajufo, DrPH, Alameda County Public Health Dept; M Lynch, Contra Costa County Dept of Public Health; JD Klausner, MD, W McFarland, MD, PhD, San Francisco Dept of Public Health; G Bell-Sanford, MSW, DV Ferrero, MPH, San Joaquin County Public Health Svcs; S Morrow, MD, San Mateo County Health Svcs Agency; K Page-Shafer, PhD, Center for AIDS Prevention Studies, Univ of California, San Francisco; G Lemp, DrPH, Universitywide AIDS Research Program, Univ of California Office of the President. Editorial Note:The population-based estimates of meth use among low-income men aged 18--35 years presented in this report support previous cross-sectional surveys linking meth use to sexual risk behaviors among heterosexual populations (2). Recent research on meth use has focused on MSM populations because of the greater prevalence of HIV in this population. Meth use was associated with increased HIV infections among MSM in San Francisco who were tested for HIV during 2001--2002 (3). Results from the study described in this report and additional data suggest that further attention should be given to the association between meth use and STD and HIV infection among heterosexuals. In southern California, 9.5% of primary and secondary syphilis cases in heterosexuals during 2004 were among persons with a history of meth use, continuing a trend of increases from 3.1% in 2001, 6.4% in 2002, and 7.3% in 2003.§ A gonorrhea outbreak in six central California counties in 2004 noted substantial meth use among heterosexual patients (men [38%], women [28%]), particularly when compared with MSM patients (8%) (MC Samuel, DrPH, California Department of Health Services, personal communication, 2005). Similar observations regarding STD incidence among MSM subpopulations (e.g., young minorities) often have indicated future trends of HIV incidence among MSM. Such projections typically have not been made for heterosexuals because of the lesser prevalence of HIV in that population. However, HIV/AIDS surveillance data from CDC and southern California indicate a growing burden of HIV among heterosexuals, particularly among females, non-Hispanic blacks, and Hispanics (8,9). Data from California HIV counseling and testing facilities also suggest the potential for meth use to connect populations with higher HIV prevalence to those with lower HIV prevalence; among bisexual males tested in California, meth users were 5.5 times more likely (99% CI = 1.4--22.3) to test HIV-positive compared with users of other stimulant drugs (CS Krawczyk, PhD, C Dahlgren, MA, unpublished data, 2002--2003). Increased HIV burden among heterosexuals, coupled with the increased use of meth nationwide and the findings of this report, suggest the potential for meth to influence heterosexual transmission of HIV. Users might initially use meth for either nonsexual (e.g., mental "escape" or weight loss) or sexual (e.g., increased sex drive, performance, and pleasure) effects; regardless of reason for use, the effects of the drug might lead to risk behaviors for transmission of STDs and HIV. In one study, 74% of male meth users reported that their sexual thoughts, feelings, and behaviors became associated with meth, 77% indicated that meth made them obsessed with having sex, and 53% said they had participated in riskier sexual acts (i.e., anal sex) while under the influence of meth (10). The findings in this report are subject to at least three limitations. First, because of the cross-sectional design of the study, no temporal or causal relations between meth use and sexual risk behaviors can be evaluated. Second, multiple data comparisons were used, increasing the potential for identifying associations by chance. Finally, because these analyses were conducted before completion of data collection, the current results might differ from the results that will be obtained by analyzing data from the entire targeted study population. The public health implications of a potential association between meth use and high-risk sexual behaviors among heterosexuals suggests the need for a broader approach in addressing meth use and risk for infection with HIV and STDs. States should consider enhancing HIV and STD prevention and treatment programs to include assessment for meth use, with referrals to meth treatment, primary meth prevention activities, and substance use treatment programs incorporating STD/HIV screening, testing, and sexual health promotion. In addition, policy initiatives should be considered to support further collaborations between professionals focusing on substance use and HIV/STDs, integrated prevention and treatment services, and research and demonstration projects evaluating the impact of treatment for meth use on sexual risk behavior reduction. Acknowledgments This report is based, in part, on data contributed by HEY-Man study team members from Alameda County Public Health Dept, Contra Costa County Dept of Public Health, San Francisco Dept of Public Health, San Joaquin County Public Health Svcs, San Mateo County Health Svcs; Center for AIDS Prevention Studies, Univ of California, San Francisco; and the Universitywide AIDS Research Program, Univ of California Office of the President. References
* Marijuana, barbiturates, cocaine, crack cocaine, heroin, or phencyclidine (PCP). † Viagra®, ecstasy, nitrites, lysergic acid diethylamide (LSD), or gamma hydroxybutyrate (GHB). § Syphilis Elimination Surveillance Data, available at http://www.dhs.ca.gov/ps/dcdc/std/mqreports.htm. Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 3/16/2006 |
|||||||||
|