|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
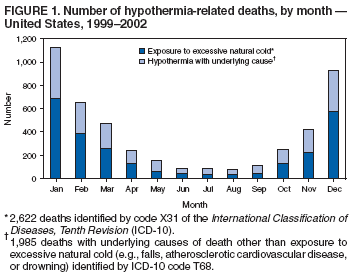
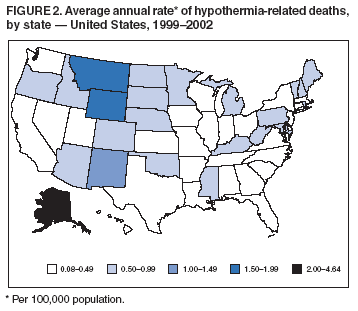
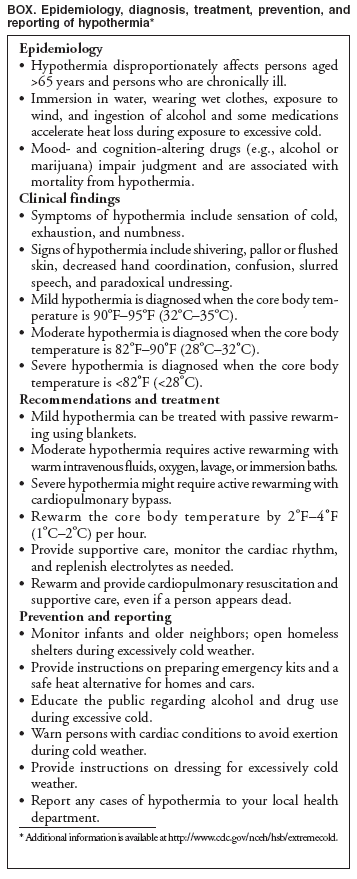
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Hypothermia-Related Deaths --- United States, 1999--2002 and 2005Hypothermia, defined as a core body temperature of <95ºF (<35ºC), is preventable. Excessive exposure to cold temperatures leads to potentially fatal central nervous system depression, arrhythmias, and renal failure (1). Advanced age, chronic medical conditions, substance abuse, and homelessness are among risk factors for hypothermia-related death. This report describes three hypothermia-related deaths that occurred during 2005 and reviews CDC data on hypothermia-related deaths during 1999--2002 in the United States. Public health strategies should target U.S. populations at increased risk for exposure to excessive cold and recommend behavior modification (e.g., dressing warmly, modifying activity levels, or avoiding alcohol) to help reduce mortality and morbidity from hypothermia. Case ReportsWyoming. In May 2005, the body of a man aged 44 years from Florida was found in Wyoming, close to a cabin, where his all-terrain-vehicle had become mired. He had rigor mortis and was pronounced dead at the scene. The man had no known medical history; however, an autopsy revealed cocaine and cannabinoids in his blood. He was partially dressed in a pullover, T-shirt, pants, and one sock. Temperatures on the preceding day ranged from 30ºF to 38ºF (-1ºC to 3ºC). The coroner certified cause of death as hypothermia resulting from exposure to cold temperatures while acutely intoxicated. New Mexico. In November 2005, the body of a woman aged 59 years was found in a field near her home in New Mexico. She was pronounced dead after attempts to revive her at a local emergency department were unsuccessful. She had a medical history of diabetes and chronic alcoholism. An autopsy revealed a vitreous humor glucose level of 410 mg/dL and a femoral blood alcohol concentration of 0.175 g/dL, more than twice the legal intoxication limit (0.08 g/dL) in New Mexico. The woman was dressed in light clothing and one shoe; her wool jacket and other shoe were found nearby. The night before the woman was found, the ambient temperature was 0ºF (-18ºC). The medical examiner certified cause of death as hypothermia resulting from exposure to excessive cold while acutely intoxicated. Alaska. In November 2005, the body of a man aged 59 years was found seated, frozen solid, at a table in his home (a converted bus) in Alaska. He was pronounced dead at the scene; he had no known medical conditions. He was inside a sleeping bag and was wearing a light jacket, long-sleeved flannel shirt, T-shirt, and pants. The temperature inside the bus was -15ºF (-26ºC), and the oil in the heater tanks was exhausted. The medical examiner certified the cause of death as hypothermia resulting from exposure to excessive cold. Risk Factors for Hypothermia-Related MortalityDuring 1999--2002, a total of 4,607 death certificates in the United States had hypothermia-related diagnoses listed as the underlying cause of death or nature of injury leading to the underlying cause of death (annual incidence: four per 1,000,000 population). Exposure to excessive natural cold (International Classification of Diseases, Tenth Revision [ICD-10] code X31) was the underlying cause in 2,622 deaths. Hypothermia (ICD-10 code T68) was the nature of injury in 1,985 deaths with underlying causes of death other than exposure to excessive natural cold (e.g. falls, atherosclerotic cardiovascular disease, or drowning). During 1999--2002, among those who died from hypothermia, 49% were aged >65 years, 67% were male, and 22% were married (compared with 52% of the overall U.S. population) (2). A high proportion (83%) of the hypothermia-related deaths occurred during October--March (Figure 1); these deaths occurred in all 50 states during 1999--2002 (range: four to 288 deaths per state), with the highest average annual rates per 100,000 population in Alaska (4.64), Montana (1.58), Wyoming (1.57), and New Mexico (1.30) (Figure 2). Most deaths were not work related (63%); 23% of affected persons were at home when they became hypothermic. Reported by: T Murphy, MD, Wyoming Dept of Health. R Zumwalt, MD, Univ of New Mexico School of Medicine, Albuquerque. F Fallico, MD, Alaska Dept of Health and Social Svcs. C Sanchez, MD, M Belson, MD, C Rubin, DVM, E Azziz-Baumgartner, MD, Div of Environmental Hazards and Health Effects, National Center for Environmental Health, CDC. Editorial Note:Hypothermia occurs when the core body temperature is <95ºF (<35ºC). If persons exposed to excessive cold are unable to generate enough heat (e.g., through shivering) to maintain a normal core body temperature of 98.6ºF (37ºC), their organs (e.g., brain, heart, or kidneys) can malfunction. When brain function deteriorates, persons with hypothermia are less likely to perceive the need to seek shelter. Signs and symptoms of hypothermia (e.g., lethargy, weakness, loss of coordination, confusion, or uncontrollable shivering) (Box) can increase in severity as the body's core temperature drops. Certain populations are at greater risk for hypothermia. Whereas U.S. Army data suggest that males and females are equally susceptible to excessive cold, most persons who die from hypothermia among civilian populations are male (3). This disparity might reflect a difference in risk-taking behavior between males and females. Older persons with preexisting medical conditions such as congestive heart failure, diabetes, or gait disturbance also are at increased risk for hypothermia because their bodies have a reduced ability to generate heat and because they are less likely to recognize symptoms of hypothermia and seek shelter from the cold. In addition, hypothermia can exacerbate certain medical conditions, with catastrophic consequences. For example, persons with cardiovascular disease can have fatal arrhythmias if their core body temperatures are <95ºF (<35ºC). Persons living in warm climates, high elevations, and areas with large daily temperature fluctuations also are at risk (4). Persons can reduce their risk for hypothermia by taking the following precautions: 1) wear a hat, mittens, and clothing that creates a static layer of warm air, provides a barrier against the wind, and keeps the body dry; 2) avoid alcohol and other mood- and cognition-altering drugs; 3) recognize the signs and symptoms of hypothermia (e.g., shivering, slurred speech, and somnolence) that indicate the need to seek shelter and call for help; and 4) keep emergency kits containing blankets, radios, noncaffeinated fluids, high-energy food, and an extra supply of medications for chronic conditions readily available. To reduce the incidence of hypothermia in the community, local health departments should implement strategies tailored to address the needs of vulnerable populations (Box). Community strategies to protect these populations include programs that check on older persons to ensure that they have heat, medications, and supplies; temporary homeless shelters; and subsidies for low-income households for heating costs. In an Alabama study, almost half of the hypothermia-related deaths occurred indoors (5). With rising energy costs, public service announcements advising persons to maintain thermostats at >60ºF might become increasingly important to prevent cases of indoor hypothermia. Acknowledgments The findings in this report are based, in part, on contributions by B Durnal, Landers, Wyoming; C McCaffrey, Wyoming Dept of Health; G Mizell, MD, North Dakota Dept of Health; and M Patel, National Center for Environmental Health, CDC. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 3/16/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|