|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
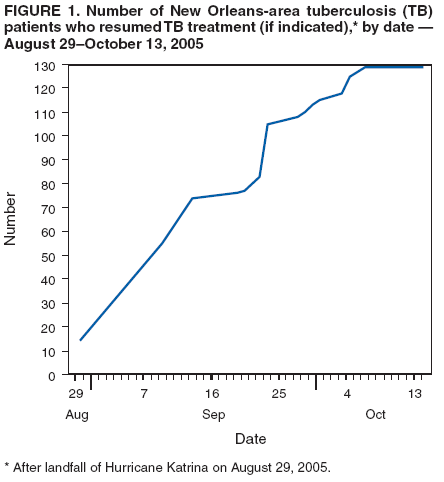
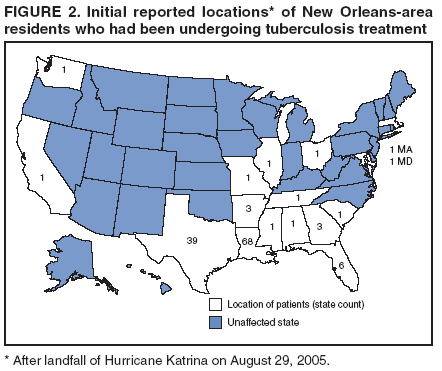
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Tuberculosis Control Activities After Hurricane Katrina --- New Orleans, Louisiana, 2005On August 29, 2005, when Hurricane Katrina struck the U.S. Gulf Coast, 130 Louisiana residents in the greater New Orleans area were known to be undergoing treatment for tuberculosis (TB) disease. Standard treatment and cure of TB requires a multidrug regimen administered under directly observed therapy (DOT) for at least 6 months (1). This report updates previous information (2) and summarizes TB cases reported as of December 31, 2005, among persons undergoing TB treatment in the New Orleans area when Hurricane Katrina made landfall and among persons who were evacuated and subsequently received a diagnosis of TB in other parts of the country. By October 13, 2005, through intensive local, state, and national efforts involving both government and private sector partners, all 130 TB patients from the New Orleans area had been located and, if still indicated, had resumed TB treatment. As a result of heightened public health surveillance among Hurricane Katrina evacuees, six other New Orleans evacuees began treatment (i.e., two persons with known TB and four with previously undiagnosed TB) after arriving in other states. The success of these post-disaster TB control measures affirms the utility of alternative data sources during health-related emergencies and the importance of maintaining a strong TB control component in the public health sector. Locating Displaced TB PatientsOn August 31, the Louisiana TB Control Program (LATB) was forced to abandon its headquarters in downtown New Orleans, and the state TB laboratory and central medication stock were located in a flooded building. Approximately half of the LATB staff had evacuated to other states, and many who stayed were temporarily displaced from their damaged homes. Although some staff members could communicate via personal cellular telephones, normal communication channels (e.g., landline telephone services or fax transmission) were disrupted. LATB began establishing a new central office approximately 100 miles away in Lafayette, Louisiana, where the state TB controller asked field staff members to submit their most recent lists of patients receiving DOT and, if known, the post-Katrina location and status of these patients. Before and after New Orleans opened for reentry on September 17, LATB staff repeatedly searched the affected parishes for known TB patients to ensure that their TB treatment continued. They visited locations known to be frequented by patients before the hurricane, called all known telephone numbers, and asked contacts whether they had heard from patients. (Similar work took place in the most affected counties of Alabama and Mississippi, where TB programs were able to account for all 48 known TB patients by September 12.) Through these frontline methods, by September 21, LATB staff identified 44 (34%) of the 130 patients who either were still residing in their homes, were temporarily living with relatives or friends in other parts of the state, or had left briefly but returned home within a few weeks post-hurricane. An additional 14 (11%) incarcerated persons remained secured in the same facilities or in other facilities where they had been transferred in anticipation of the hurricane; all 14 continued TB treatment without interruption. Beginning September 2, the national network of TB control programs took several measures to provide assistance. The TB Program of the Texas Department of State Health Services arranged for sputum specimens from Louisiana to be processed through the Texas State Laboratory. VersaPharm Incorporated, a pharmaceutical supplier, sent LATB free shipments of replacement TB medications. To help with state-to-state communication, the National TB Controllers Association and the CDC Division of Tuberculosis Elimination established a Katrina TB help desk in Atlanta, Georgia. TB programs in other states could telephone the help desk to inquire whether an evacuee in their jurisdiction who reported taking TB medication was on the list of New Orleans-area patients who remained missing. If so, the help desk facilitated completion of the standard TB interjurisdictional transfer form for public health authorities in the new state of residence. Through this process, an additional 34 (26%) displaced New Orleans-area patients were located by September 21. Novel approaches were then used to locate the 38 remaining New Orleans-area patients. Public registries (e.g., an online hospital patient locator and an online locator coordinated by the American Red Cross) were searched for information on patients, leading to contact with an additional six patients (5%). Agreements and other arrangements were established with relief agencies and targeted national pharmacy chains to permit limited cross-matching of missing patients' names while safeguarding their privacy and confidentiality. Twenty-six (20%) patients were located through relief agency rosters, and the final six (5%) were located through searches of recent prescription activity in other states. By October 13, 2005, all 130 New Orleans-area patients had been located and had resumed TB treatment, if still indicated (Figure 1). Sixty-eight (52%) of the patients had stayed in Louisiana, 39 (30%) had relocated to Texas, and the remaining 23 (18%) had relocated to 14 other states (Figure 2). Health departments in these states assumed responsibility for the TB case management of displaced persons for as long as the patients remained in their new jurisdictions. Two additional New Orleans evacuees who had received pulmonary TB diagnoses before the hurricane but had not started treatment began DOT in Arkansas and Colorado. In the months after the hurricane, many displaced Louisiana residents returned; 96 (74%) of the 130 persons who had been receiving treatment for TB had returned to the greater New Orleans area by December 31. Detection and Treatment of New TB Cases Among EvacueesStaff at the Katrina TB help desk also coordinated activities to identify evacuees who might have undiagnosed cases of TB disease (3). Detecting new TB cases and bringing them to the attention of local or state TB controllers as early as possible was critical to preventing transmission of Mycobacterium tuberculosis; initiation of effective treatment rapidly reduces infectiousness (4). As of December 31, four new TB cases among Hurricane Katrina evacuees from Louisiana had been verified and reported by other states (California, Connecticut, Pennsylvania, and Texas). Reported by: C DeGraw, G Kimball, R Adams, T Misselbeck, R Oliveri, J Plough, TB Control Section, Louisiana Office of Public Health, Louisiana Dept of Health and Hospitals. C Wallace, PE Cruise, TB Program, Texas Dept of State Health Svcs. C Pozsik, National TB Controllers Assoc. Epidemiology Elective Program, Office of Workforce and Career Development; Office of the Director, National Center for HIV, STD, and TB Prevention; Div of TB Elimination, National Center for HIV, STD, and TB Prevention, CDC. Editorial Note:Ensuring successful treatment of TB is an essential public health responsibility carried out daily by TB control programs in health departments across the United States. This report describes the challenges faced by LATB when Hurricane Katrina completely disrupted its normal operations. Despite the challenges, persistent frontline work by staff (who themselves had suffered the consequences of Hurricane Katrina) helped ensure continuity of TB treatment for all 130 patients, including not only those who stayed but also those who relocated to 15 other states. During an initial disaster response, the most urgent public health priorities are providing safe and adequate shelter, water, food, and sanitation. Also important are interventions to minimize potential spread of infectious diseases, including TB, as displaced persons congregate in shelters and resettle in new communities. All TB control programs should consider planning for emergencies that might result in mass displacement of patients. In response to the lessons learned from Hurricane Katrina, the TB programs in Louisiana and Texas took several measures in advance of Hurricane Rita to ensure continuity of care: 1) preparing line lists of patients in parishes and counties that might be affected, 2) giving patients a 2-to-4 week supply of medication in case DOT was interrupted, 3) ensuring that patients had a list of phone numbers to reestablish contact with the health department if they were displaced, 4) obtaining contact information for patients' relatives and friends in other parts of the country, 5) ensuring that back-up copies of patient records were available for potential sharing with new jurisdictions, and 6) moving essential TB supplies and medication stock to safer inland areas. These activities contributed to continuity of TB treatment after landfall of Hurricane Rita on September 24, 2005. Locating patients who could not be found by traditional field methods required cross-matching their names and other limited identifying data with records maintained by relief agencies and national pharmacy chains. This approach, although valuable, required a substantial effort to negotiate and execute event-limited agreements and arrangements that addressed privacy and confidentiality concerns and applicable matters related to the Health Insurance Portability and Accountability Act, Standards for Privacy of Identifiable Health Information (HIPAA Privacy Rule) and related laws.* Prearranged agreements of this type, applicable to various health-related emergencies, would have facilitated faster location of patients. Further efforts to standardize electronic health records and secure HIPAA-compliant platforms for sharing information among public health and private entities could facilitate locating TB patients in future disasters (5). After Hurricane Katrina, multiple Louisiana TB patients were displaced to other states, requiring mobilization of the existing national network of state and local TB control programs not directly affected by Hurricane Katrina. This network, under guidance of the National TB Controllers Association and with assistance from the CDC Division of Tuberculosis Elimination, coordinated activities to account for all TB patients who had been evacuated. Such accomplishment affirms the importance of maintaining strong TB control programs in the public health sector. Acknowledgments This report is based on contributions by the following state and local health departments: Alabama; Arkansas; Los Angeles, California; Denver, Colorado; Colorado; Norwalk, Connecticut; Connecticut; Florida; Georgia; Suburban Cook County, Illinois; Illinois; Maryland; Massachusetts; Mississippi; Missouri; Ohio; Philadelphia, Pennsylvania; Pennsylvania; South Carolina; Tennessee; Houston, Texas; Corpus Christi-Nueces County, Texas; Dallas County, Texas; Galveston County, Texas; Harris County, Texas; Tarrant County, Texas; Snohomish, Washington; and Washington; the MetroHealth Medical Center TB Clinic, Cleveland, Ohio; and Div of Emergency Operations, Coordinating Center for Terrorism Preparedness and Emergency Response; Coordinating Center for Health Information and Service; Office of the Chief Science Officer, Office of the Director; and Office of the General Counsel, Office of the Director, CDC. References
* The HIPAA Privacy Rule generally applies to entities covered by the Rule, known as "covered entities." These covered entities include health-care providers who bill electronically, health-care insurers, and health-care clearinghouses. Under the Rule, CDC is not a covered entity but rather a "public health authority." Covered entities are permitted to disclose protected health information to a public health authority, subject to certain conditions. In addition, CDC is subject to federal privacy laws that govern the use and disclosure of certain identifiable records. Although not required, data-sharing agreements might be appropriate in certain instances of cross-matching to document compliance with applicable law and ensure appropriate procedural and security protections for the information exchanged.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 3/29/2006 |
|||||||||
|