|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
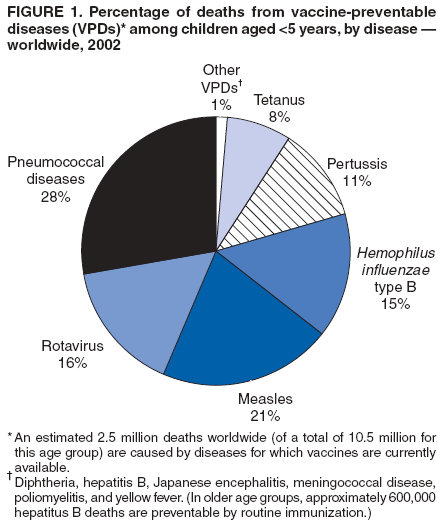
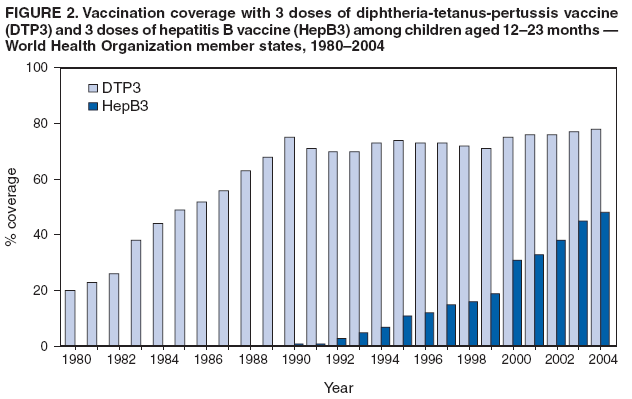
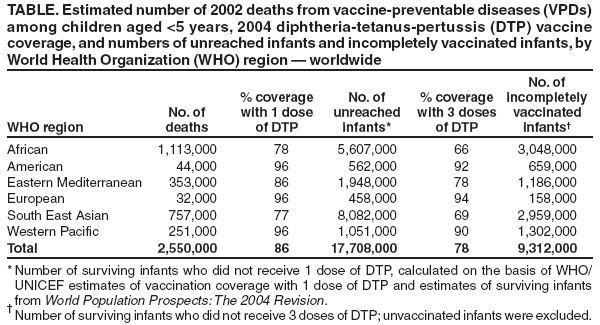
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Vaccine Preventable Deaths and the Global Immunization Vision and Strategy, 2006--2015Immunization is among the most successful and cost-effective public health interventions (1,2). Immunization programs have led to eradication of smallpox, elimination of measles and poliomyelitis in regions of the world, and substantial reductions in the morbidity and mortality attributed to diphtheria, tetanus, and pertussis. The World Health Organization (WHO) estimates that 2 million child deaths were prevented by vaccinations in 2003 (3). Nonetheless, more deaths can be prevented through optimal use of currently existing vaccines. This report summarizes estimates of deaths attributed to vaccine-preventable diseases (VPDs) and vaccination coverage by WHO region and outlines the Global Immunization Vision and Strategy developed by WHO and the United Nations Children's Fund (UNICEF) and partners for implementation during 2006--2015. Estimates of Vaccine-Preventable Deaths, 2002, and Recommended VaccinesMortality estimates can be used to prioritize public health interventions. For VPDs, these estimates indicate the number of deaths that could be averted if existing vaccines were used to their fullest potential. In 2002, among diseases for which vaccines are universally recommended, WHO estimates that fewer than 1,000 children aged <5 years died from polio; 4,000 children died from diphtheria; 15,000 children died from yellow fever; 198,000 children died from tetanus; 294,000 children died from pertussis; 386,000 children died from Hemophilus influenzae type b (Hib); and 540,000 children died from measles (4). Among adults, 600,000 deaths were attributed to hepatitis B virus infections, the majority of which were acquired in childhood. In addition, other diseases can be prevented by vaccines that are not universally recommended by WHO. During 2002, the largest numbers of deaths from these VPDs among children aged <5 years were attributed to pneumococcal disease (716,000) and rotavirus infection (402,000) (4) (Figure 1); 240,000 adult deaths were attributed to human papilloma virus infection (WHO, unpublished data, 2002). During 2002, approximately 1.9 million (76%) of the 2.5 million VPD deaths among children aged <5 years worldwide occurred in Africa or Southeast Asia (Table). Vaccines for measles, polio, diphtheria, pertussis, and tetanus have been part of the WHO recommended vaccination series since the inception of the Expanded Programme on Immunization in 1974. In 1988, WHO recommended inclusion of yellow fever vaccine in routine infant immunization programs in countries with populations at risk for yellow fever. Hepatitis B vaccine was universally recommended for infants by WHO in 1992; in 1998, WHO recommended that Hib vaccine be included in routine infant immunization programs, where suited to national capacities and priorities. In January 2006, the WHO Immunization Strategic Advisory Group recommended global implementation of Hib vaccination unless robust evidence exists of low disease burden or overwhelming impediments to implementation exist (5). WHO has not issued a universal recommendation for pneumococcal vaccine. The only licensed pneumococcal conjugate vaccine does not contain serotypes 1 and 5, which are responsible for a substantial proportion of severe disease in developing countries. Vaccines containing these and additional serotypes are under development. Where the control of invasive pneumococcal disease is considered a public health priority and where available vaccine serotypes match the most important local serotypes, WHO recommends that the conjugate vaccine should be considered for inclusion in childhood vaccination programs. One rotavirus vaccine has been licensed in the United States since February 2006, and another is currently licensed in more than 36 countries outside the United States; nonetheless, no WHO universal recommendation has been issued for rotavirus vaccine because this vaccine is relatively new and vaccine efficacy data have not been established in all WHO regions. Human papilloma virus vaccine is under review by the Food and Drug Administration for licensure in the United States and is not licensed outside the United States. Estimated Vaccination Coverage, 2004By convention, the success of routine immunization programs in reaching children has been measured by the vaccination coverage achieved with the third dose of diphtheria-tetanus-pertussis vaccine (DTP3) among children aged 12--23 months (6). WHO and UNICEF base estimates of routine vaccination coverage for all diseases (including DTP3) on review of administrative coverage data, surveys, national reports, and consultation with local and regional experts (7). Aggregated across member states, routine coverage with DTP3 ranged from 70% to 78% during 1990--2004 (Figure 2). Substantial differences exist in DTP3 coverage among WHO regions. The European, Western Pacific, and American regions had DTP3 coverage of >90% in 2004, whereas coverage was 69% in the South East Asia region and 66% in the African region. Poor coverage in a region contributes to a high burden of disease and is reflected in the number of child deaths (Table). Prevention of hepatitis B virus infection is assessed by vaccination coverage with the third dose of hepatitis B vaccine (HepB3) among children aged 12--23 months. As of 2004, a total of 153 (80%) of 192 WHO member states were using the vaccine. Of these 153 countries, 102 (67%) had HepB3 coverage of >80%, 36 (24%) had coverage of <80%, and 15 (10%) either had not reported coverage data or had not introduced the vaccine nationwide. Overall vaccination coverage with HepB3 is increasing and had reached 48% of WHO member states in 2004 (Figure 2). Prevention of Hib infection also is assessed by vaccination coverage with the third dose of the vaccine (Hib3). Ninety-two (48%) of the WHO member states have introduced Hib vaccine since 1986; in 2004, a total of 78 (85%) reported Hib3 coverage of >80% among children aged 12--23 months. Global Immunization Vision and StrategyIn 2005, WHO and UNICEF worked with partners to create a Global Immunization Vision and Strategy (GIVS) for 2006--2015 (8,9). This strategy, which seeks to expand the reach of vaccination to every eligible person (3), is intended to be used as the basis for developing national comprehensive multiyear plans. GIVS articulates the WHO and UNICEF visions for global immunization in 2015 and is composed of four strategic areas: 1) protecting more persons in a changing world by improving routine immunization coverage, ensuring at least four immunization contacts per child, and expanding immunization programs to all ages; 2) introducing new vaccines and technologies; 3) integrating immunization, other linked health interventions, and surveillance in the health systems context; and 4) creating global partnerships to support and finance immunizations (3). Reported by: Dept of Immunization, Vaccines, and Biologicals, World Health Organization, Geneva, Switzerland. United Nations Children's Fund, New York, New York. Global Immunization Div, National Center for Immunization and Respiratory Diseases (proposed); M McMorrow, MD, EIS Officer, CDC. Editorial Note:Despite the successes of immunization programs worldwide, global estimates of VPD mortality and DTP3 coverage underscore that available vaccines are not being used to their fullest potential. Challenges include sustaining current vaccination coverage levels, extending vaccination to unreached populations and persons beyond infancy, and introducing new vaccines and technologies. GIVS provides a framework within which these challenges can be addressed. Implementation of multiple activities outlined in GIVS actually began before development of this strategic vision. However, GIVS unifies these activities and, by serving as the basis for national comprehensive multiyear plans, provides countries with a method for identifying critical areas and resource needs, and an opportunity to track their national progress. At least 40 countries are developing these multiyear plans, which will include cost estimates for all immunization activities and outline future initiatives to improve vaccine coverage and extend vaccination to unreached populations (WHO, unpublished data, 2006). Fifty-three countries have implemented the Reaching Every District (RED) strategy, WHO's key strategy for increasing routine vaccination coverage. The RED strategy encourages supportive supervision, regular outreach services, community links with service delivery, improved data management, and improved planning based upon data (3). Increasing access to new vaccines has the potential to greatly reduce the number of child deaths worldwide. Two GIVS priorities are to help countries develop the capacity to make informed decisions regarding vaccine introduction on the basis of robust evidence of disease burden, economic analysis, and feasibility of introduction, and to ensure that national systems can sustain vaccine delivery programs. In 2005, a Hib initiative funded by the Global Alliance for Vaccines and Immunization (GAVI)* was launched to help countries decide whether to introduce Haemophilus influenzae type b vaccine into their immunization programs. GAVI-funded initiatives also exist for planning future introduction of pneumococcal and rotavirus vaccines. The GIVS acknowledges the need to strengthen the health sector to decrease barriers to immunization, improve disease surveillance, and strengthen data management and suggests strategies for implementation. Furthermore, because immunization services often have the greatest community penetration of any public health intervention, the GIVS encourages linking immunizations to other interventions rather than providing them in isolation. For example, vitamin A supplements have been distributed through immunization services since 1987; during 2004, a total of 73 countries provided vitamin A to infants with routine immunizations, immunization campaigns, or both. In addition, during 2005, three immunization campaigns in Africa distributed antihelminthic medications and nine African countries distributed insecticide-treated mosquito bednets during immunization campaigns or routine services. Pilot projects also are in development to assess integration with routine immunization services of medical care for infants exposed to human immunodeficiency virus and intermittent preventive therapy against malaria for infants. Various global partnerships and funding mechanisms are available to sustain immunization programs. For example, GAVI offers financial support to introduce new and underused vaccines, improve injection safety, and strengthen routine immunization services. In addition, the International Finance Facility for Immunization,† a United Kingdom initiative, uses legally binding, long-term commitments from donors to leverage funding from international capital markets by issuing bonds to increase the funds available for immunization programs. By using the framework of the GIVS, WHO, UNICEF, and partners are continuing to develop plans of action within each of the strategic areas outlined above. In collaboration with WHO, CDC is assisting in the development of guidelines for integrated surveillance for all vaccine-preventable diseases. CDC will continue to provide technical support to WHO and UNICEF as requested to support the GIVS. References
* GAVI is an alliance of public and private sector organizations that supports introduction of new vaccines through administration of the Vaccine Fund. GAVI also has been active in improving routine immunization program services and data quality and increasing support for vaccination globally. Additional information is available at http://www.gavialliance.org. † Additional information is available at http://www.iffim.com. Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 5/11/2006 |
|||||||||
|