|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
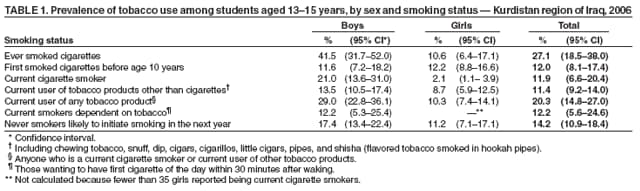
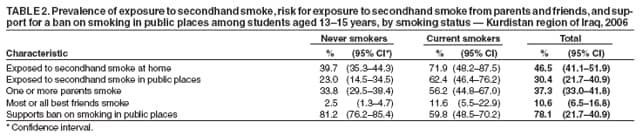
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Tobacco Use Among Students Aged 13--15 Years --- Kurdistan Region, Iraq, 2005Tobacco use is one of the major preventable causes of premature death and disease in the world. The Global Youth Tobacco Survey (GYTS), part of the Global Tobacco Surveillance System initiated by the World Health Organization (WHO), CDC, and the Canadian Public Health Association, was developed to monitor tobacco use, attitudes about tobacco, and exposure to secondhand smoke among youths and has been conducted in 140 countries (1,2). This report presents findings from the GYTS conducted in the Kurdistan region of Iraq (i.e., Irbil, as-Sulaymaniyah, and Dahuk governorates) in 2005, which revealed that one in 10 students currently smoked cigarettes or used other tobacco products. Boys (21%) were statistically significantly more likely than girls (2.1%) to smoke cigarettes, but no significant difference was observed between boys and girls in their use of other tobacco products. Public health authorities in the Kurdistan Region of Iraq can use the baseline information from the GYTS to design and implement tobacco-control programs to reduce youth smoking. GYTS is a school-based survey that collects data from students aged 13--15 years by using a standardized methodology for constructing the sample frame, selecting participating schools and classes, and processing data. GYTS uses a two-stage, cluster-sample design that produces representative samples of students in grades associated with ages 13--15 years (2). In the Kurdistan region of Iraq, this age range is covered by the first through fourth years of secondary education; the GYTS sampling frame included all schools containing these grades from the governorates of Irbil, as-Sulaymaniyah, and Dahuk. At the first sampling stage, the probability of a school's being selected was proportional to the number of students in that school enrolled in the target grades. At the second stage, classes within the selected schools were selected randomly. Students attending school in the selected classes on the day the survey was administered were eligible to participate. In total, 1,989 students completed the GYTS (58.1% male and 41.9% female). The school response rate was 100% (25 schools), the student response rate was 95.6%, and the overall response rate (i.e., the school rate multiplied by student rate) was 95.6%. This report presents data on the following indicators: prevalence of lifetime cigarette smoking, age of initiation of cigarette smoking, prevalence of current cigarette smoking, prevalence of tobacco dependency among current smokers (i.e., desire to have a cigarette first thing in the morning), prevalence of current tobacco use other than cigarettes, likelihood of never smokers beginning to smoke within the next year (i.e., susceptibility index) (3), prevalence of direct exposure to secondhand smoke at home and in public, and prevalence of potential exposure to secondhand smoke from parents and best friends who smoke. A weighting factor was applied to each student's record to adjust for the probability of selection at the school and class levels and for nonresponse rates at the school, class, and student levels. A final adjustment summed the weights by grade and sex to the population of school children in the first through fourth years of secondary education. Statistical software was used to account for the complex survey design and to compute standard errors and 95% confidence intervals for the estimates. Two-tailed t tests were used to establish significant differences. Only significant differences (p<0.05) are reported. The results of this analysis indicated that 27.1% of Kurdistan students in the grades surveyed had ever smoked cigarettes and that boys (41.5%) were significantly more likely than girls (10.6%) to have ever smoked (Table 1). Approximately one in every 10 ever smokers of both sexes initiated smoking before age 10 years. Slightly more than one in 10 students currently smoked cigarettes (11.9%) or currently used other tobacco products (11.4%). Boys (21.0%) were significantly more likely than girls (2.1%) to smoke cigarettes currently. Two in 10 students (20.3%) currently used any tobacco product, with the rate for boys (29.0%) significantly higher than that for girls (10.3%). Results also demonstrated that 12.2% of current smokers who were boys wanted to have a cigarette within 30 minutes of waking each morning and that 14.2% of never smokers indicated they were likely to initiate smoking in the next year, with no significant difference between boys and girls. However, for girls the proportion of never smokers likely to initiate smoking (11.2%) was significantly higher than the current smoking rate (2.1%). Exposure to secondhand smoke was significantly higher among students who currently smoked cigarettes than among never smokers both at home (71.9% versus 39.7%) and in public places (62.4% versus 23.0%). A significantly higher percentage of current smokers also had parents who smoked (56.2% versus 33.8%) and best friends who smoked (11.6% versus 2.5%); never smokers were significantly more likely than current smokers to favor a ban on smoking in pubic places (81.2% versus 59.8%) (Table 2). Reported by: D Barzani, MD, JS Sarhang, MD, Ministry of Health, Kurdistan Regional Government, Iraq. F El-Awa, PhD, Eastern Mediterranean Regional Office, World Health Organization. CW Warren, PhD, NR Jones, PhD, S Asma, DDS, Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion; LR McKnight, PhD, EIS Officer, CDC. Editorial Note:The findings in this report indicate that tobacco-control program in the Kurdistan region of Iraq faces the several challenges. First, although boys were significantly more likely than girls to be current smokers (21.0% versus 2.1%), this difference might be changing soon because the likely rate of smoking initiation among never smokers was nearly as high among girls (11.2%) as among boys (17.4%). The susceptibility index, used to measure likely initiation of smoking among never smokers, has been shown to be a good predictor of future smoking behavior (3). Second, the prevalence of any current tobacco use (20.3%) is only slightly less than the sum of the prevalence of current cigarette smoking (11.9%) and the prevalence of other current tobacco use (11.4%), indicating that few students are using both cigarettes and other tobacco products at the same time. This observation suggests that the Kurdistan tobacco-control program should address all forms of tobacco use. Other tobacco use in the Kurdistan region primarily involves the use of shisha (i.e., flavored tobacco smoked in hookah pipes), and the 8.7% rate of smoking shisha in hookah pipes among girls is a concern. Third, the high rate of student exposure to secondhand smoke indicates a need for further measures to pass and enforce laws governing smoking in public places. Creating smoke-free areas and educating the public about the dangers of secondhand smoke likely will have a complementary effect by reducing the social acceptance of tobacco use around persons who do not smoke (4). The Ministry of Health (MOH) in the Kurdistan region of Iraq has established a tobacco-control unit and made tobacco control a priority among health-care workers and youths. MOH also has begun training programs for health professionals on tobacco control and cessation and has initiated a health education campaign directed toward youths (5). In addition, a health-education campaign to be conducted in schools throughout the Kurdistan region during the 2006--07 academic year will include antismoking posters and pamphlets. Kurdistan law bans smoking in all government buildings, including schools and administrative office buildings of MOH and the Ministry of Education (MOE). MOH will convene a tobacco-control meeting in November 2006 to bring together representatives from MOH, MOE, and the Ministry of Higher Education to discuss the findings from GYTS and to plan development of a comprehensive tobacco-control program. The findings in this report are subject to at least three limitations. First, because the sample surveyed was limited to youths attending school, it might not be representative of all adolescents aged 13--15 years in the Kurdistan region of Iraq. According to MOE, the enrollment rate (i.e., the percentage of all eligible youth enrolled in secondary schools) in the region is 82% (Kurdistan regional government, MOE, unpublished data, 2006). Second, these data were based on responses of those students who were in school on the day of the survey and who completed the survey. However, the effect of this limitation is likely minimal because 100% of randomly selected schools and 95.6% of all eligible students in those schools participated. Finally, the data are based on self-reports of students, who might underreport or overreport their behavior or attitudes. Although the extent of this possible bias cannot be determined from the Iraq Kurdistan region GYTS, responses to tobacco-related questions on U.S. surveys similar to the GYTS have demonstrated good test-retest reliability (6). Systematic global surveillance of youth tobacco use is the essential first step in preventing the worldwide epidemic of death and disease that smoking is projected to cause in the 21st century (7). The GYTS enhances the capacity of countries to develop, implement, and evaluate their tobacco-control programs. MOH now has baseline data on youth tobacco use and attitudes toward tobacco use that likely will help to develop a comprehensive tobacco-control program. GYTS should be repeated every 3--4 years to evaluate the effectiveness of such a program. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 5/25/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|