|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
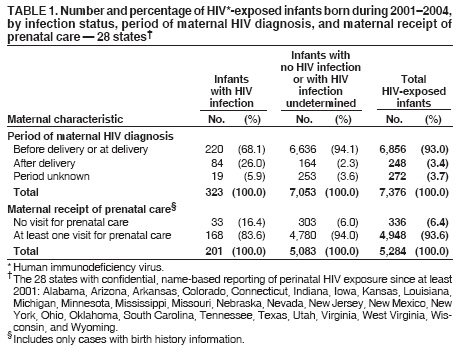
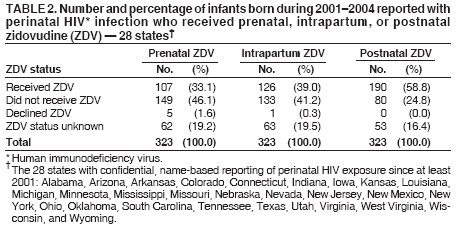
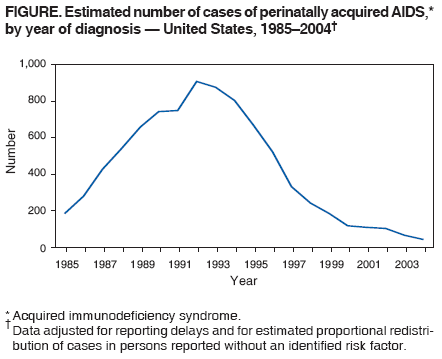
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Achievements in Public Health: Reduction in Perinatal Transmission of HIV Infection --- United States, 1985--2005During 2005, an estimated 92% of acquired immunodeficiency syndrome (AIDS) cases reported among children aged <13 years in the United States were attributed to mother-to-child transmission of human immunodeficiency virus (HIV) (CDC, unpublished data, 2006). Transmission can occur during pregnancy, labor, delivery, or breastfeeding. Estimates of the number of perinatal HIV infections peaked in 1991 at 1,650 (1) and declined to an estimated range of 144--236 in 2002 (CDC, unpublished data, 2006). This reduction is attributed to routine HIV screening of pregnant women, use of antiretroviral (ARV) drugs for treatment and prophylaxis, avoidance of breastfeeding, and use of elective cesarean delivery when appropriate. With these interventions, rates of HIV transmission during pregnancy, labor, or delivery from mothers infected with HIV have been reduced to less than 2% (2), compared with transmission rates of 25%--30% with no interventions (3). Despite these gains, substantial challenges to reducing perinatal transmission of HIV remain. Every perinatal HIV infection represents a sentinel health event, often indicating a woman who had undiagnosed HIV infection before pregnancy or did not receive appropriate interventions to prevent transmission of the virus to her infant. Therefore, to strengthen and sustain measures to maximally reduce perinatal transmission, public health activities should give high priority to collection of data to identify where missed opportunities occur and target prevention efforts accordingly. Trends in Perinatal HIV/AIDSAIDS cases. Pediatric AIDS cases were reported as early as 1982 (4) . The estimated number of perinatally acquired AIDS cases in the United States peaked at 945 in 1992 (Figure) and declined rapidly with expanding prenatal testing and implementation of appropriate preventive interventions. In 2004, an estimated 48 perinatally acquired cases of AIDS were reported (5), a decrease of approximately 95% from 1992. In 2004, approximately 38% of perinatally acquired AIDS cases were reported in children aged <1 year. As with adults, reporting of children with AIDS underestimates the current burden of HIV infection in children. HIV cases. Because not all states conduct name-based HIV-infection reporting,* estimates of HIV infections among children over time are more uncertain than for AIDS cases. Availability of highly active antiretroviral therapy (HAART) has changed the progression time to AIDS; therefore, using reported AIDS cases to estimate HIV cases among children has been more difficult in recent years. Previous estimates placed the peak of HIV-infected infants at approximately 1,650 in 1991, followed by a steep decline (6). A similar procedure, which did not produce a point estimate, yielded a range of 284--367 for the estimated number of HIV-infected infants born in 2000 (7). More recent estimates have used perinatal HIV data from 35 states† with confidential, name-based HIV reporting of pediatric HIV infections since at least 2002 to extrapolate proportionately, on the basis of perinatal AIDS cases, to the entire U.S. population. Using this procedure, an estimated 144--236 HIV-infected infants were born in the United States in 2002 (CDC, unpublished data, 2006). The precision of perinatal HIV case estimates should improve as additional states adopt name-based HIV-infection reporting. Milestones in the Reduction of Perinatal HIV TransmissionHIV testing. The observed decreases in pediatric AIDS and HIV cases likely resulted primarily from increased identification of infected mothers and exposed infants and timely intervention to prevent perinatal HIV transmission (1). The need for pregnant women to know their HIV status was recognized early in the epidemic as a key step to preventing perinatal transmission. In 1985, CDC recommended that pregnant women in groups at high risk be offered counseling and voluntary HIV testing (8). At the time, risk-based screening for HIV was recommended because no treatment was available for HIV infection; however, many women with HIV infection were not identified by risk-based screening. In 1995, after a clinical trial determined that zidovudine (ZDV) was able to reduce perinatal HIV transmission (3), CDC and the American Academy of Pediatrics (AAP) recommended universal voluntary counseling and HIV testing for all pregnant women to allow timely prophylactic use of ZDV (9,10). In 1999, the Institute of Medicine reported that the lack of timely HIV diagnosis in pregnant women was the largest contributor to continued perinatal transmission in the United States (11) and recommended universal HIV screening of pregnant women with patient notification and the ability to decline screening (i.e., the opt-out approach). AAP and the American College of Obstetricians and Gynecologists (ACOG) published a joint statement in 1999 recommending universal opt-out HIV screening for pregnant women (12). CDC testing guidelines in 2001 recommended routine HIV screening as early as possible during pregnancy for all pregnant women with streamlined counseling and consent processes to reduce barriers to testing (13), and in 2003, a letter from CDC to U.S. health professionals also recommended the opt-out screening approach (14). Despite such measures, from 2001 to 2004, nearly 7% of HIV-infected pregnant women reported from 28 states with confidential, name-based perinatal HIV exposure reporting since at least 2001 had HIV that remained undiagnosed by the time of delivery (Table 1). However, the majority of these women delivered in hospital settings, where they might be tested. In 2001, CDC recommended rapid or expedited testing for all women during labor and delivery with undocumented HIV status (13). With the approval of a rapid HIV test by the Food and Drug Administration (FDA) in 2002, providing testing for women with undocumented HIV status in labor became more feasible. Such testing allows provision of interventions to reduce the risk for transmission of HIV infection even in the absence of treatment during pregnancy. In 2004, the Mother-Infant Rapid Intervention at Delivery study demonstrated that rapid testing was acceptable and feasible in the delivery setting (15), and ACOG also expanded its recommendations to include rapid testing for women in labor with unknown HIV status (16). As HIV testing during pregnancy became more routine, some areas (e.g., New York state) documented an increasing proportion of neonatal HIV infections transmitted by women who tested HIV negative earlier in pregnancy (17). In response, ACOG and CDC recommended a routine second HIV test during the third trimester for women known to have elevated risk for HIV infection (e.g., history of sexually transmitted disease [STD] or illicit drug use) and in areas with elevated HIV prevalence among women of childbearing age (13,16). Although nationally representative data on prenatal HIV testing rates do not exist, in four states the proportion of HIV-infected pregnant women in whom HIV infection was diagnosed before giving birth increased from 68% in 1993 to 81% in 1996 (18). Recently, among all HIV-exposed infants reported to CDC through the HIV/AIDS Reporting System (HARS) (i.e., from 28 states with confidential, name-based perinatal HIV exposure reporting for infants who were born during 2001--2004), 93% of mothers had known HIV status before or at the births of their infants (Table 1). Antiretroviral use. In February 1994 the Pediatric AIDS Clinical Trials Group (PACTG) 076 trial demonstrated a breakthrough prevention intervention with a 67% reduction in perinatal HIV transmission by using a three-part regimen consisting of administration of ZDV to the mother during pregnancy, intravenous ZDV during labor, and ZDV to the infant for 6 weeks (3). In April 1994, CDC issued provisional guidelines for ZDV use to reduce perinatal transmission (19), and, in July 1994, FDA approved ZDV for this use. In August 1994, the U.S. Public Health Service Task Force (USPHSTF) and CDC issued consensus recommendations for use of this regimen to reduce perinatal HIV transmission (20). In the late 1990s, additional ARV medications were developed and licensed, and administration of HAART became the standard of care, which usually consists of three or more drugs used in combination to inhibit viral replication at multiple steps of the replication cycle. Such therapy is capable of reducing viral replication to levels undetectable by available assays. In 1998, USPHSTF and CDC recommended HAART for pregnant women who required the therapy for their own health and recommended that all HIV-infected pregnant women be offered combination therapy, while acknowledging uncertainty about benefits and risks to the fetus (21). Subsequent studies determined that maternal treatment with HAART reduced perinatal transmissions to <2% of deliveries by women with HIV; the risk of mother-to-child transmission was independently correlated with the complexity of ARV therapy (i.e., the number and types of different medications) and with maternal HIV RNA levels (2). Current guidelines recommend use of HAART (including ZDV whenever possible) for women who require it for their own health and for all women whose plasma HIV RNA levels are >1,000 copies/mL and also recommend that such therapy be considered instead of ZDV alone for women with plasma HIV RNA levels <1,000 copies/mL (22). Certain less complex regimens, administered only intrapartum and postnatally to infants, also have been shown to reduce perinatal transmission, although to a lesser extent than when antepartum therapy also was administered (23). Such regimens are recommended in the United States when the mother has not received ARV prophylaxis during pregnancy, such as women first identified during labor as infected with HIV (22). Some evidence from in vitro and in vivo models has suggested the potential for teratogenic or carcinogenic effects from some ARV agents in pregnancy (24). However, analysis of all prospective cases reported to the Antiretroviral Pregnancy Registry during January 1989--July 2005 identified no detectable increase in overall risk of birth defects or of specific birth defects in humans (25). Toxicity related to mitochondrial dysfunction has been reported in patients receiving long-term treatment with nucleoside analogs; infants exposed to these agents should be regularly monitored for the development of such toxicity (22). Data are conflicting regarding whether receipt of combination ARV therapy in pregnancy is associated with other adverse pregnancy outcomes, such as preterm birth; all pregnant women receiving such therapy and their infants should receive monitoring for pregnancy complications and potential toxicity (22). The use of ARV drugs for prevention of perinatal HIV transmission increased dramatically after 1994. A four-state (Louisiana, Michigan, New Jersey, and South Carolina) study determined that, during 1993--1996, the proportion of HIV-infected pregnant women offered prenatal ZDV increased from 27% to 85%, the proportion offered intrapartum ZDV increased from 5% to 75%, and the proportion offered neonatal ZDV increased from 5% to 76% (18). In 24 areas conducting enhanced perinatal HIV surveillance during 1999--2001, nearly 79% of HIV-infected pregnant women received some ARV therapy during pregnancy; 77% received ARV therapy during the intrapartum period, and 92% of HIV-exposed infants received some form of ARV therapy (26). In the Women and Infant Transmission Study, the rate of perinatal transmission decreased from 22.6% in 1990, when most women received no ARV therapy or only ZDV for treatment of HIV infection, to 1.2% in 2003, when 87% received combination therapy (2; L Mofenson, MD, National Institutes of Health, personal communication, 2006). Avoidance of breastfeeding. In 1985, breastfeeding was reported as potentially associated with mother-to-child transmission of HIV (27), and HIV was isolated from breast milk (28). That year, CDC recommended that women with HIV infection avoid breastfeeding (8). Subsequent international studies estimated that one third to one half of perinatal HIV transmission among breastfeeding populations occurred during breastfeeding (29). Avoidance of breastfeeding is now recommended in areas, including the United States, where safe alternatives are reliably accessible and affordable (30). Scheduled cesarean delivery. Several studies have confirmed that cesarean delivery performed before onset of labor and membrane rupture can reduce HIV transmission to infants whose mothers do not receive ARV therapy during pregnancy or who receive only ZDV (31,32). Rates of cesarean delivery among HIV-infected pregnant women in one large cohort study increased from 20% to 44% after presentation of the results of these studies in 1998 (33). However, the efficacy of cesarean delivery in women who have received potent combination therapy and have low HIV RNA levels (<1,000 copies/mL) remains unclear (22,31,32). The uncertain benefit for prevention of perinatal HIV transmission is likely outweighed by the potential risks of operative delivery in such women, given that the risk for HIV transmission is less than 2%. USPHSTF recommends that scheduled cesarean delivery be offered to women with HIV RNA levels >1,000 copies/mL near the time of delivery (22). Current ChallengesThe decreases in perinatal HIV infections and perinatally acquired AIDS cases in the United States represent an important achievement in public health. However, perinatal transmission of HIV continues to occur. Infant infections can be associated with interruptions of care at any stage for HIV-infected women and their infants. Females aged >13 years accounted for only 7% of reported new AIDS cases in 1985 (CDC, unpublished data, 2006) but 27% of reported cases in 2004 (5). Enhanced primary HIV-prevention strategies are needed to prevent new infections in women, which will, in turn, prevent perinatal HIV infections. Lack of prenatal care for HIV-infected women also contributes to ongoing perinatal transmission. Data from HARS for births during 2001--2004 indicate that 16% of mothers of HIV-infected infants had no documented prenatal care visits (Table 1), excluding cases where no infant birth history information was available. For many HIV-infected women, mental health or substance use concerns and HIV-related stigma present barriers to prenatal care (34). Increasing accessibility to prenatal care services is crucial to sustain and maximize the decline in perinatal HIV infections. Pregnant women also might have increased susceptibility to HIV infection (35), and infection of women during pregnancy might lead to a substantial number of perinatal transmissions (17). In addition to universal HIV screening as early as possible in pregnancy, CDC now recommends a second HIV test during the third trimester for populations of women with elevated HIV incidence and rapid HIV testing for women in labor with undocumented HIV status (13). Requirements for lengthy HIV-prevention counseling and written documentation of informed consent for HIV testing might present additional barriers to routine prenatal testing (7). Among the 28 states with perinatal HIV-exposure and HIV/AIDS reporting through HARS, during 2001--2004, approximately 26% of mothers of HIV-infected infants were not recognized as infected with HIV before delivery (Table 1). Testing rates often are higher in areas employing opt-out testing for pregnant women, compared with opt-in strategies that require specific written documentation of informed consent for HIV testing (36). Many HIV-infected women and their infants still do not receive appropriate ARV treatment and prophylaxis. Of all HIV-infected infants reported to HARS during 2001--2004 from 28 states with confidential, name-based infant HIV-exposure reporting, 46% had not received prenatal ZDV (Table 2), 41% had not received ZDV during labor and delivery, and 25% had not received postnatal ZDV. Many of these infant infections could have been prevented if the HIV infections of their mothers had been identified through adequate preconception and prenatal care and if appropriate prophylactic interventions had been administered. Maximal reduction of perinatal HIV infection is one of the four primary goals of CDC's Advancing HIV Prevention initiative, announced in 2003 (37). CDC perinatal HIV-prevention programs currently focus on five key areas: 1) implementation of rapid HIV testing in labor and delivery for women with undocumented HIV status; 2) social marketing efforts to increase awareness of the need for HIV testing among pregnant women; 3) outreach efforts to promote receipt of prenatal care by pregnant women; 4) case management services to promote receipt of prenatal care and receipt of appropriate medication and interventions among HIV-infected pregnant women; and 5) provider training to increase availability of rapid testing services. Programs are also underway to increase collaboration between perinatal HIV programs and programs addressing other important perinatal infections. In addition, CDC continues to monitor infections among children and adults and produces periodic surveillance reports to provide data for public health decision makers. To monitor perinatal HIV-prevention measures and address missed opportunities for prevention, CDC and the Council of State and Territorial Epidemiologists recommend that all states require public health reporting of all cases of perinatal HIV exposure in infants. Implementation of recommendations for universal prenatal HIV testing, ARV prophylaxis, elective cesarean delivery, and avoidance of breastfeeding has resulted in a 95% decrease in the number of perinatal AIDS cases in the United States since 1992 and a decline in the risk for perinatal HIV transmission from an HIV-infected mother to less than 2%. However, barriers to the elimination of perinatal HIV infection remain, as the number of HIV infections continues to rise among women, and health-care services are not universally accessed by women in need of these services. Finally, the success in reducing perinatal HIV transmission observed in the United States contrasts with the situations in poorer countries, particularly in sub-Saharan Africa, where perinatal HIV transmission remains largely unabated. Continued success in the United States and reduction of perinatal HIV transmission in areas where such transmission remains common will require sustained commitment to prevention of HIV infection among women and to treatment for women affected by HIV/AIDS. Reported by: L Mofenson, MD, Pediatric, Adolescent, and Maternal AIDS Br, Center for Research for Mothers and Children, National Institute of Child Health and Human Development, National Institutes of Health. AW Taylor, MD, M Rogers, MD, M Campsmith, DDS, NM Ruffo, J Clark, MPH, MA Lampe, MPH, AK Nakashima, MD, S Sansom, PhD, Div of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD and TB Prevention (proposed), CDC. References
* As of May 2006, the following areas conducted name-based HIV-infection reporting for children: Alabama, Alaska, American Samoa, Arizona, Arkansas, California, Colorado, Connecticut, Delaware, Florida, Georgia, Guam, Idaho, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maine, Michigan, Minnesota, Mississippi, Missouri, Nebraska, Nevada, New Hampshire, New Jersey, New Mexico, New York, North Carolina, North Dakota, Northern Mariana Islands, Ohio, Oklahoma, Pennsylvania, Puerto Rico, South Carolina, South Dakota, Tennessee, Texas, U.S. Virgin Islands, Utah, Virginia, Washington, West Virginia, Wisconsin, and Wyoming. † Alabama, Alaska, Arizona, Arkansas, Colorado, Connecticut, Florida, Idaho, Indiana, Iowa, Kansas, Louisiana, Michigan, Minnesota, Mississippi, Missouri, Nebraska, Nevada, New Jersey, New Mexico, New York, North Carolina, North Dakota, Ohio, Oklahoma, Pennsylvania, South Carolina, South Dakota, Tennessee, Texas, Utah, Virginia, West Virginia, Wisconsin, and Wyoming.
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 6/1/2006 |
|||||||||
|