 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Nonfatal Injuries and Restraint Use Among Child Passengers --- United States, 2004During 1978--2004, annual rates of child fatalities from motor vehicle crashes (MVCs) declined from 31.8 to 22.3 deaths per million. This decline might be partially attributed to the increased use of both child safety seats (for infants and young children) and seatbelts (for older children) (1). Nevertheless, among child passengers aged <12 years in 2004, nearly 1,200 children died (1), and an estimated 180,000 were injured and treated in U.S. hospital emergency departments (EDs) (2). Recent studies suggest that MVC fatalities and injuries among infants and children can be reduced further by promoting and enforcing age-appropriate restraint use (3). The National Electronic Injury Surveillance System-All Injury Program (NEISS-AIP) provides data on all injury-related hospital ED visits (4). For this report, NEISS-AIP was expanded to collect additional information about injuries and restraint use for child passengers aged <12 years involved in MVCs during 2004 and examined at 15 U.S. EDs. Of the children injured in MVCs, 45% were either not restrained or inappropriately restrained. Most inappropriate restraint use occurred among children aged 4--8 years who were placed prematurely in seatbelts. The percentage of unrestrained children who were hospitalized was three times that of restrained children. Restraint use for child passengers should be promoted vigorously and enforced because it can reduce their risks for multiple injuries and hospitalization from MVCs. NEISS-AIP, maintained by the Consumer Product Safety Commission (CPSC), is a nationwide, stratified probability sample of hospitals that provides information on injury-related ED visits (4). NEISS-AIP routinely collects data that include 1) demographic information; 2) injury information, including the injury event, location, intent, and mechanism; and 3) medical information abstracted from ED charts (i.e., principal diagnosis, primary affected body part, treatment date, and ED discharge disposition). Hospitals are divided into five strata, four based on size (i.e., reported annual numbers of ED visits) and one stratum consisting of children's hospitals. A stratified random sample of 15 hospitals (three per stratum) was selected for this study from among the 50 NEISS-AIP hospitals that provided patient identifiers to CPSC for follow-up interviews. For these selected hospitals, NEISS-AIP data were expanded for 2004 by 1) collecting information for up to five injury diagnoses and affected body parts from ED records for children aged <12 years injured in MVCs and 2) interviewing parents about their child's restraint use and crash circumstances. This study was conducted with the approval of CDC's Institutional Review Board. Restraint use was classified as unrestrained or restrained. For restrained children, appropriateness of restraint type was based on age, weight, and parent-reported height using child passenger safety guidelines from the National Highway Traffic Safety Administration (NHTSA) (5). The guidelines state that 1) children should remain in rear-facing infant seats until they weigh >20 pounds and are aged 1 year, at which point they may be placed in forward-facing child safety seats; 2) children weighing >40 pounds may be placed in booster seats until they are aged >9 years or >57 inches tall, at which point they may wear lap/shoulder belts; and 3) children should not be placed in lap belts only (i.e., without shoulder belts). This analysis used children's weights recorded in ED charts when available (for 272 children) and parent-reported weights when chart-reported weights were missing (for 323 children); children's weights were not available from either source for 40 children. In addition, this analysis assumed that 69 children aged <8 years with missing heights were <57 inches tall, on the basis of growth charts for U.S. children (6), which report that 97% of children aged 7 years are <52 inches tall. The missing heights for two children aged 8 years in lap/shoulder belts were kept as "missing." For the 1,370 children aged <12 years seen for injuries attributed to motor vehicles at the 15 participating EDs, CPSC contacted 911 households (66%). Of these 911 households, 738 (81%) agreed to participate; 649 (88%) child passengers in MVCs were eligible for this study. Restraint use was unknown for 14 children (2%). A total of 635 children were known to be either restrained (n = 578) or unrestrained (n = 57) (Table 1). Eight percent of children aged <3 years, 6% aged 4--6 years, 10% aged 7--8 years, and 11% of children aged >9 years were unrestrained. Restraint use was similar for boys and girls. Among children whose race/ethnicity was known, the percentages of unrestrained black and Hispanic children were at least six times those of non-Hispanic whites (12% and 14%, respectively, versus 2%). The percentage of children in trucks who were unrestrained was three times that of those riding in other types of vehicles (24% versus 8% on average for cars, sports-utility vehicles, and vans). Eighty-one percent of children had a single-injury diagnosis, whereas 16%, 3%, and 0.8% had two, three, and four diagnoses, respectively. Eight percent of children required hospital admission. The percentage of unrestrained children with multiple diagnoses was nearly twice that of restrained children (30% versus 18%). The percentage of unrestrained children requiring hospitalization was almost three times that of restrained children (21% versus 7%). Appropriateness of restraint type could be determined for 573 of 578 restrained children; 342 (59%) were restrained appropriately, and 231 (40%) were restrained inappropriately (Table 2). Appropriateness of restraint type was unknown for five children (1%) because of missing data. Of those inappropriately restrained, 177 (77%) were children aged 4--8 years who were inappropriately wearing seatbelts. Of these 177, a total of 139 (79%) were wearing lap/shoulder belts, and 38 (21%) were wearing lap belts only. Eighty-nine (61%) of the 147 children aged 4--6 years and 87 (86%) of the 101 children aged 7--8 years were placed prematurely in seatbelts. One child aged 8 years, who was tall enough to wear a seatbelt, was restrained inappropriately in a lap belt only. Appropriateness of restraint type was similar for boys and girls. A higher percentage of both black and Hispanic children were inappropriately restrained, compared with non-Hispanic whites (47% and 50%, respectively, versus 34%). A higher percentage of children in trucks were restrained inappropriately, compared with children in other vehicle types (48% versus 40% on average for cars, sports-utility vehicles, and vans). Reported by: RA Shults, PhD, A Greenspan, DrPH, A Dellinger, PhD, Div of Unintentional Injury Prevention, T Haileyesus, MS, Office of Statistics and Programming, National Center for Injury Prevention and Control; KC Lee, MD, EIS Officer, CDC. Editorial Note:The results of this study underscore the need for restraint use for child passengers, which can reduce their risks for multiple injuries and hospitalization in MVCs. The findings in this study also are consistent with previous studies reporting that young children who should be in booster seats are often placed in seatbelts, including lap/shoulder and lap belts (3,7,8). Previous studies have indicated that young children are at increased risk for serious injury when placed in seatbelts prematurely (3,8). Likely mechanisms include 1) increased head excursion, resulting in its impact with the child's knees or the vehicle interior or 2) rapid "jackknife" bending about an improperly fitted seatbelt, which increases risks for intraabdominal and spinal cord injuries (injuries known collectively as "seatbelt syndrome") (8). The findings in this report are subject to at least five limitations. First, these findings rely, in part, on parental reports of crash circumstances and their children's restraint use, heights, and weights, which might be subject to social desirability bias, particularly for restraint use. Although some discrepancies were observed between chart-reported and parent-reported weights for the 257 children who had data from both sources, they were well-correlated (correlation coefficient = 0.96, p<0.0001). Second, certain children aged <8 years with missing heights might have actually been >57 inches tall, so this analysis might have assumed incorrectly that they were not tall enough for lap/shoulder belts. Third, crash circumstances were not verified independently or investigated. Fourth, generalizability of this study's findings might be limited by its low response rate, small sample size, and missing data for race/ethnicity. Finally, individual ED health-care providers might vary in how thoroughly they record diagnosis information. Child restraint laws in all 50 states should be updated to be consistent with current NHTSA guidelines and vigorously enforced. Booster seat use should be promoted for children who have outgrown child safety seats but have not yet reached the appropriate age or height for wearing lap/shoulder belts. Although 33 states and the District of Columbia have laws requiring booster seat use for such children, only two states (Tennessee and Wyoming) require their use for children aged up to 8 years. Strong enforcement measures, targeted mass media campaigns, and community outreach can increase age-appropriate restraint use among children (9). Community-based interventions to increase age-appropriate child restraint use should target groups with higher rates of nonuse of restraints (e.g., blacks, Hispanics, and truck passengers) and inappropriate restraint use (e.g., premature graduation to lap/shoulder belts and use of lap belts only). Two of the national health objectives for 2010 include reduction in deaths from MVCs and increased restraint use for child passengers (10). Child passenger safety also has been identified as a research priority by CDC, which conducts research, supports extramural research and programs, and disseminates information regarding safe practices. Acknowledgments The findings in this report are based, in part, on contributions by the Consumer Product Safety Commission and L Annest, PhD, Office of Statistics and Programming, National Center for Injury Prevention and Control, CDC. References
Table 1 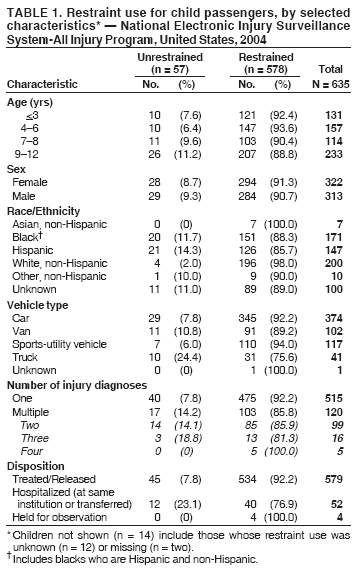 Return to top. Table 2 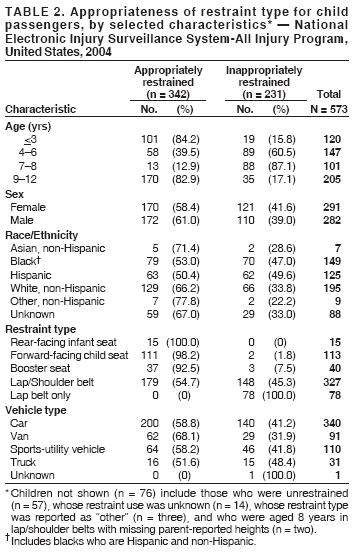 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 6/7/2006 |
|||||||||
|