|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
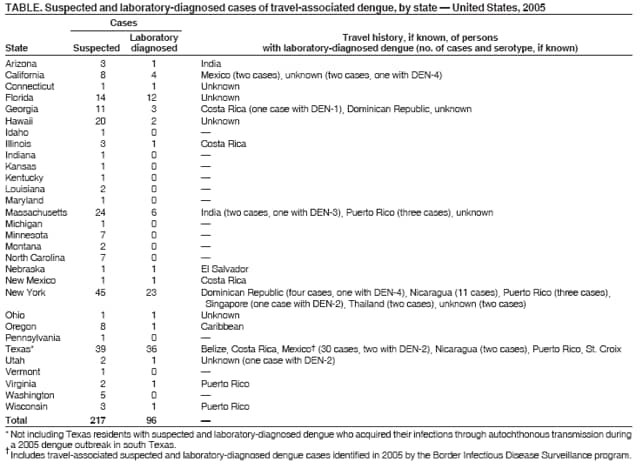
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Travel-Associated Dengue --- United States, 2005Dengue is a mosquito-transmitted, acute viral disease caused by any of four dengue virus serotypes (DEN-1, DEN-2, DEN-3, or DEN-4). Dengue is endemic in most tropical and subtropical areas of the world and has occurred among U.S. residents returning from travel to such areas (1,2). In collaboration with state health departments, CDC maintains a passive surveillance system for travel-associated dengue among U.S. residents. Suspected dengue in travelers is reported to state health departments, which forward specimens to CDC for diagnostic testing.* A case of travel-associated dengue is defined as laboratory-diagnosed dengue in a resident of one of the 50 states or the District of Columbia (DC) who traveled to a dengue-endemic area outside the United States or DC any time during the 14 days before symptom onset. This report summarizes information regarding 96 travel-associated dengue cases, including one fatality, among U.S. residents during 2005. Travelers to tropical areas can reduce their risk for dengue by using mosquito repellent and avoiding exposure to mosquitoes. Health-care providers should consider dengue in the differential diagnosis of febrile illness in patients who have returned recently from dengue-endemic areas. Serum samples from 199 travelers with suspected dengue on the basis of clinical symptoms (3) during 2005 were submitted to CDC from 30 states. Of these 199 patients, 78 (39%) received a laboratory diagnosis of dengue, 51 (26%) were classified as indeterminate because a convalescent-phase sample for serologic testing was unavilable, and 70 (35%) did not have dengue. Of the 78 patients with dengue, 70 (90%) had elevated anti-dengue IgM antibodies, and eight (10%) had a dengue virus identified in serum by either polymerase chain reaction or viral isolation. Eighteen additional patients (12 from Florida, five from Texas, and one from New Mexico) had elevated anti-dengue IgM antibodies identified by commercial laboratories and also received a diagnosis of dengue (Table). Of the 96 total patients with a dengue diagnosis, 53 (55%) were female. The median age of the 83 patients for whom age was reported was 43 years (range: <1--84 years). Travel destinations of 73 (76%) patients were identified. Thirty-two (44%) reported travel to Mexico during the 2 weeks before illness onset, 19 (26%) to Central America, 16 (22%) to the Caribbean, and six (8%) to Asia. Clinical symptoms were reported for 24 (25%) patients. Six had at least one hemorrhagic symptom (e.g., epistaxis, hematemesis, hematuria, hemoptysis, petechia, or purpura). Of the 96 patients, 17 (18%) were reported to have been hospitalized, including one who died. This rare travel-associated dengue fatality occurred in a woman aged 28 years in otherwise good health who had recently returned from a week in Mexico. Reported by: A Ayala, MPH, A Rivera, MS, M Johansson, J Muñoz, PhD, Div of Vector-Borne Infectious Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases (proposed); M Ramos, MD, H Mohammed, PhD, EIS officers, CDC. Editorial Note:Dengue viruses are transmitted to humans by certain species of Aedes mosquitoes. The majority of U.S. residents who contract dengue become infected during travel to tropical and subtropical areas outside of the 50 states and DC, although autochthonous transmission has been documented in Texas (4,5) and Hawaii (6). Nearly as many cases of travel-associated dengue were identified in 2005 (96 cases) as were identified during the preceding 5 years combined (98 cases) (1,2). The incidences of dengue and dengue hemorrhagic fever (DHF) are increasing in the tropical areas of the world, including in the Western hemisphere (7). Waning support for mosquito-control programs (i.e., less funding for vector control), urbanization in the tropics, increasing human populations, and increased use of nonbiodegradable products (i.e., which can hold fresh rain water and provide places for mosquitoes to lay eggs) have all contributed to the recent resurgence of dengue (7). In 2005, outbreaks of dengue and DHF were reported from several areas in the Americas, including Mexico, Puerto Rico, the U.S. Virgin Islands, Guadeloupe, Martinique, Belize, El Salvador, Costa Rica, Nicaragua, Ecuador, Venezuela, and Brazil.† The incubation period for dengue ranges from 3 to 14 days. Dengue virus infection can be asymptomatic or cause illness ranging from mild, undifferentiated fever to severe disease that includes hemorrhage and shock (8). DHF is characterized by fever, minor or major bleeding manifestations, thrombocytopenia (<100,000 platelets/µL), and evidence of increased vascular permeability (e.g., hemoconcentration [hematocrit >20% higher than baseline], pleural or abdominal effusions, or hypoproteinemia) (6). Dengue shock syndrome (DSS) also can occur; DSS is DHF with signs of circulatory failure, including narrow pulse pressure (<20 mm Hg), hypotension, or shock and has a case-fatality rate of approximately 10% (9). However, with early diagnosis and appropriate treatment, the case-fatality rate can be reduced to less than 1% (10). Aspirin and other nonsteroidal antiinflammatory drugs are contraindicated for patients with dengue because of their anticoagulant properties. The findings in this report are subject to at least two limitations. First, these data are likely subject to underreporting because the surveillance system is passive (i.e., relies on health-care providers to report infections), and dengue is not a nationally notifiable disease in the United States. Second, travel histories and clinical information were not available for all cases, and the available data might not be representative of all persons with travel-associated dengue. Persons traveling to areas where dengue is endemic should avoid exposure to mosquitoes by using repellents, wearing protective clothing, and remaining in well-screened or air-conditioned areas. Preventing travel-associated dengue not only benefits the traveler but also helps prevent introduction of dengue virus into areas of the United States (primarily the southeastern states) where vector mosquitoes might transmit the virus indigenously. No vaccine is available for preventing dengue infection. Health-care providers should consider dengue in the differential diagnosis of patients who have fever and a history of travel to tropical areas any time during the 2 weeks before symptom onset. To diagnose dengue, health-care providers should obtain from the patient both an acute-phase (0--5 days after symptom onset) serum sample for directly detecting dengue virus and a convalescent-phase serum sample for detecting anti-dengue antibody, preferably obtained 1--2 weeks after the first sample.§ Serum samples obtained for viral identification and serologic diagnosis can be sent through state or territorial health departments to CDC's Dengue Branch, Division of Vector-Borne Infectious Diseases, National Center for Infectious Diseases, 1324 Calle Cañada, San Juan, Puerto Rico 00920-3860; telephone, 787-706-2399; fax, 787-706-2496. Serum samples should be accompanied by a summary of clinical and epidemiologic information, including date of disease onset, date of sample collection, and detailed recent travel history. Additional information regarding dengue case reporting and instructions for specimen shipping are available at http://www.cdc.gov/ncidod/dvbid/dengue/dengue-hcp.htm. Acknowledgments This report is based, in part, on data contributed by state and local health departments and technical assistance from P Collins, Div of Vector-Borne Infectious Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases (proposed), CDC. References
* Some cases are confirmed by commercial laboratories and reported to CDC by state health departments without requests for further diagnostic testing. † Data from International Society for Infectious Diseases (ProMED-mail, the Program for Monitoring Emerging Diseases, available at http://www.promedmail.org) and CDC (Epidemic Information Exchange [Epi-X], available at http://www.cdc.gov/epix). § Although serologic testing can detect diagnostic levels of anti-dengue IgM antibody reliably for approximately 30 days after symptom onset (and for 2--3 months in some cases), the optimum timing for a convalescent-phase sample is 1--2 weeks after the first sample.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 6/29/2006 |
|||||||||
|