|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
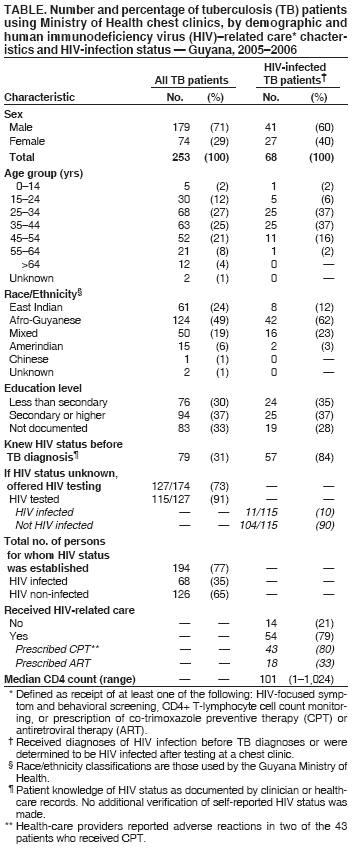
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. HIV Counseling, Testing, and Care of Tuberculosis Patients at Chest Clinics --- Guyana, 2005--2006Tuberculosis (TB) is a leading cause of morbidity and mortality among persons living with human immunodeficiency virus (HIV) or acquired immunodeficiency syndrome (AIDS) (1). During 2004, Guyana had an estimated TB incidence rate of 140 per 100,000 population (1), the fourth highest rate in the Americas (after Haiti, Bolivia, and Peru); Guyana also had an estimated adult HIV prevalence of 2.5% (2), and 20% of TB patients were reported to be infected with HIV (3). In 2000, the Guyana Ministry of Health (MOH) began providing HIV counseling, testing, and referrals to HIV/AIDS programs at its six public chest clinics.* At the end of 2005, chest clinics also began providing co-trimoxazole preventive therapy (CPT) to HIV-infected TB patients as a measure against common opportunistic infections. During February--June 2006, an international team† assessed the extent to which MOH chest clinics in Guyana had implemented these interventions during July 2005--June 2006. This report summarizes the results of that assessment, which determined that, among 253 TB patients sampled, 174 (69%) initially did not know their HIV-infection status; 127 (73%) of those patients were offered HIV counseling and testing, and 115 (91%) accepted and were tested for HIV. Of the 115 who were tested, 11 (10%) were determined to be HIV infected; overall, 68 (35%) of the 194 patients whose HIV-infection status was known were HIV infected (i.e., 11 who were tested at the chest clinics plus 57 with preexisting knowledge of their HIV status). These results indicate both a high rate of HIV infection among TB patients in Guyana and the ability of chest clinics to provide HIV-related interventions in resource-limited settings. In Guyana, approximately 90% of all reported TB cases are diagnosed and patients treated at the six MOH chest clinics (3). These clinics provide on-site rapid HIV testing and, with the exception of one facility, are located on the same campus or within 1 kilometer of MOH's HIV clinics. Chest clinics currently do not prescribe antiretroviral therapy (ART) to TB patients who are HIV infected, although this is planned for the future. When possible, however, chest clinics employ clinicians trained in both TB and HIV patient care. All patients starting TB treatment at the chest clinics during July--December 2005 whose health-care records (e.g., patient medical records, treatment cards, or registers and logs at chest and HIV clinics) were located were included in the evaluation. Data on patient demographics, diagnosis, laboratory tests, and treatment were collected. TB disease was defined using World Health Organization (WHO) laboratory or clinical case definitions (4). HIV-related care was defined as receipt of at least one of the following: symptom screening for HIV-related complications, CD4+ T-lymphocyte cell count monitoring, or provision of CPT or ART. During the 6-month evaluation period, 380 patients were registered as starting TB treatment at the six chest clinics. Of these, health-care records for 253 (67%) patients were located and available for review. Similar to most resource-limited settings, Guyana's MOH chest clinics do not use electronic medical records or formal record-tracking systems, hindering attempts to locate patient records. The median age of the TB patients was 38 years (range: 9 months--82 years). Seventy-nine (31%) of the 253 patients reported knowing their HIV-infection status before starting TB treatment and were not retested for HIV (Table). Of the remaining 174 patients with unknown HIV status before diagnosis of TB, 127 (73%) were offered HIV counseling and testing, and 115 (91%) of the 127 agreed to be tested. Eleven (10%) of those tested were HIV infected. The 47 (27%) patients with unknown HIV status who were not offered HIV counseling and testing were less likely to have had a secondary education (prevalence odds ratio [POR]: 4.6, 95% confidence interval [CI] = 1.5--15.0, p<0.01) and more likely to be aged >44 years (POR: 11.0, CI = 2.4--99.0, p<0.01) than those offered HIV testing. Among the 194 patients for whom HIV status was determined, 68 (35%) were HIV infected (57 who self-reported their HIV serostatus before starting TB treatment and 11 who had been tested for HIV infection at the chest clinics). Documentation of HIV-related care was available for 54 (79%) of the 68 HIV-infected patients. Among these 54 patients, 38 (70%) had a recent CD4+ T-lymphocyte cell count recorded, 43 (80%) had been prescribed CPT, and 18 (33%) had been prescribed ART (Table). Patients not documented as receiving ART either were not referred to or did not comply with referral to an HIV clinic, did not meet national criteria for ART initiation, refused ART initiation, or had HIV clinic medical records that were unavailable for review (i.e., their MOH HIV clinic records were not located or they received HIV-related care at a private facility). Rates of CPT use did not differ significantly by patient sex, race/ethnicity, age group, or education level. Reported by: S Persaud, MBBS, J Mohanlall, MBBS, Ministry of Health, Guyana. M Bateganya, MD, C Anude, MD, Guyana office of the Francois-Xavier Bagnoud Center/Univ of Medicine and Dentistry of New Jersey. C La Fleur, MD, Canadian Society for International Health. TH Holtz, MD, CD Wells, MD, Div of Tuberculosis Elimination; A DuBois, MD, S Filler, MD, Div of Global AIDS, National Center for HIV, Viral Hepatitis, STDs, and Tuberculosis Prevention (proposed); S Chideya, MD, EIS Officer, CDC. Editorial Note:According to WHO recommendations, 1) HIV testing and counseling should be offered to all TB patients in settings where the HIV prevalence among TB patients exceeds 5%; 2) TB control programs should establish a referral linkage with HIV/AIDS programs to provide a continuum of care and support for persons living with HIV/AIDS who are receiving or who have completed their TB treatment; and 3) TB and HIV/AIDS programs should establish a system to provide CPT to eligible persons living with HIV/AIDS who have active TB (5). The assessment described in this report demonstrated that of the TB patients using Guyana's MOH chest clinics for whom HIV status was determined, 35% were HIV infected, and 79% of these patients received varying types of HIV-related care; in addition, 73% of those who did not know their HIV status upon arrival at the chest clinic were offered HIV counseling and testing. These findings support the usefulness of chest clinics in the initiation and maintenance of HIV-related interventions in resource-limited settings. The chest clinics provided HIV counseling and testing to 73% of eligible TB patients, which compares well with published rates for other countries where HIV prevalence among TB patients exceeds 5% (1,6--8). Comparable reports regarding provision of HIV-related care by chest clinics in other countries have not been published. Although these clinics had the capacity to provide HIV counseling and testing and HIV-related care, 27% of TB patients met national Guyana guidelines for receipt of HIV counseling and testing (i.e., had unknown HIV infection status) but were not documented as receiving these interventions. Discrepant rates of HIV counseling and testing by demographic characteristics (i.e., age and education level) were noted. Further study might be considered to determine what factors (e.g., communication or cultural) might have resulted in older TB patients and those with less education being less likely to be offered HIV counseling and testing. Strengthening the observance of national guidelines regarding HIV counseling and testing (in addition to CPT use and referrals to HIV/AIDS programs) to include all persons, regardless of demographics, is critical. In addition, because one third of eligible patient records could not be located during this assessment, improving current medical record filing and tracking systems likely would improve patient management. The findings in this report are subject to at least five limitations. First, data were missing from patient records at all six chest clinics, and 33% of patient records were not available; whether the HIV-related characteristics of these patients differed significantly from the sampled group is unknown. Second, 27% of patients with unknown HIV status at the time of TB diagnosis were not offered HIV counseling and testing; whether the proportion of HIV infection in this patient group differed significantly from those who were tested is unknown. Third, patient reports of receiving HIV-related health care from private providers were not verified. Fourth, self-reports of HIV status could not be confirmed for some patients (i.e., those not visiting MOH HIV clinics). Finally, MOH chest clinics did not begin providing CPT to HIV-infected TB patients until the end of 2005. HIV-infected patients who completed most or all of their TB-related care before chest clinic distribution of CPT might have lower rates of use. Because HIV-related care is available to patients without cost in Guyana, adoption of routine diagnostic HIV testing for all persons visiting chest clinics (i.e., "opt-out" testing) should be considered, including for persons unable to provide documentation of their HIV status. Routine testing could increase the detection of HIV infections and enable more HIV-infected TB patients to receive HIV-related care. In addition, training should be provided regularly to chest clinic staff members to underscore the importance of observing national TB and HIV guidelines. Further integrating TB and HIV control measures (e.g., by including in Guyana's National HIV Registry those HIV-infected patients who received their diagnoses at chest clinics and who receive HIV-related care at non-MOH facilities) could provide additional safeguards for patient follow-up and appropriate health care. * The public health-care facilities in Guyana responsible for diagnosing TB infection in patients and managing their disease. † Team members included Guyana MOH, the Guyana office of the Francois-Xavier Bagnoud Center/University of Medicine and Dentistry of New Jersey, the Canadian Society for International Health, and CDC. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 8/10/2006 |
|||||||||
|