|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
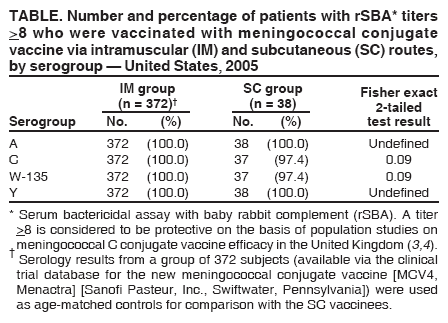
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Inadvertent Misadministration of Meningococcal Conjugate Vaccine --- United States, June--August 2005During June--August 2005, CDC and the Food and Drug Administration (FDA) were notified of seven clusters of inadvertent subcutaneous (SC) misadministration of the new meningococcal conjugate vaccine (MCV4, Menactra) (Sanofi Pasteur, Inc., Swiftwater, Pennsylvania), which is licensed for intramuscular (IM) administration only. A total of 101 persons in seven states were reported to have received MCV4 by the SC route. Of these, 100 were contacted by their health-care providers and advised of the administration error. CDC conducted an investigation to determine whether SC administration of MCV4 resulted in a protective immunologic response. This report describes the results of that investigation, which indicated that, despite the misadministration, persons vaccinated by the SC route were sufficiently protected and that revaccination was not necessary. In 1978, the meningococcal polysaccharide vaccine (MPSV4, Menomune) (Sanofi Pasteur) was licensed in the United States for administration by the SC route. The newer MCV4 is a tetravalent meningococcal conjugate vaccine that was licensed in January 2005 on the basis of immunogenic noninferiority to MPSV4 and demonstrated safety (1). Both vaccines protect against Neisseria meningitidis serogroups A, C, Y, and W-135. Because immunogenicity and safety of MCV4 were assessed for IM administration only, the vaccine is licensed for IM use only. The immunogenicity and safety of MCV4 after SC administration were not evaluated. CDC contacted the providers who inadvertently misadministered the vaccine to inform them of the investigation. Providers contacted the vaccinees to advise them of the error and invite them to participate in the investigation. Twelve nonserious adverse events* were reported among 54 persons from whom providers solicited such information. Eleven events were local reactions, including injection-site rash, tenderness, swelling, induration, or pain, and one was a fever of 1 day's duration. The frequency and nature of adverse events among these persons are similar to those reported after IM vaccination in MCV4 licensure trials (1). Providers collected single serum samples from 21 to 105 days after vaccination from 38 SC vaccinees who agreed to participate (response rate: 38%). Serology results from a group of 372 subjects available from the manufacturer's prelicensure MCV4 clinical trial database, with serum samples collected 21 to 42 days after IM vaccination, were used as age-matched controls for comparison with the SC vaccinees. Age-matched comparison of rSBA response was conducted because of the effect of age on serologic response to MCV4. Immune responses for each vaccine serogroup (A, C, Y, and W-135) were measured by serum bactericidal assay using baby rabbit complement (rSBA). Serologic testing of the SC vaccinees was performed by the same laboratory using the same methods used to test the IM vaccinees from the MCV4 clinical trial. Geometric mean titers (GMTs) of SC vaccinees were compared with those of age-matched IM vaccinees from the MCV4 clinical trials. Titers of individual vaccinees were evaluated for each vaccine serogroup to determine whether the vaccinees developed a protective response as a result of the SC vaccination; rSBA titers >8 were considered protective (2,3). For each of the four vaccine serogroups, the proportion of SC vaccinees with rSBA titers >8 was >97% and did not differ significantly (by Fisher exact test) from the proportion of IM vaccinees with rSBA titers >8 (Table). Two patients vaccinated by the SC route had rSBA titers <8 (one participant for serogroup C only and one for serogroup W-135 only). GMTs were significantly lower for SC vaccinees compared with age-matched IM vaccinees for serogroups A, C, and Y (odds ratios = 1.78 [95% confidence interval (CI) = 1.21--2.62]; 2.27 [CI = 1.33--3.89]; and 1.66 [CI = 1.03--2.67], respectively); however, no significant difference was observed between GMTs for serogroup W-135 (odds ratio = 0.71 [CI = 0.45--1.14]). On the basis of the protective rSBA titer results for nearly all of SC vaccinees participating in this investigation, revaccination was not recommended. Reported by: S Shadomy, DVM, B Plikaytis, PhD, National Center for Zoonotic, Vector-Borne, and Enteric Diseases (proposed); T Clark, MD, G Carlone, PhD, N Messonnier, MD, National Center for Immunization and Respiratory Diseases (proposed); K Uhde, PhD, K Winger, DVM, EIS officers, CDC. Editorial Note:The most likely reason for the inadvertent misadministration of MCV4 described in this report was that the older meningococcal vaccine, MPSV4, in use for nearly 30 years, is licensed for SC administration, whereas MCV4 is licensed only for IM administration. This reason was cited by health-care providers participating in the investigation. Although the overall serologic response for SC vaccinees was lower than that of IM vaccinees as determined by GMTs, nearly all persons vaccinated by the SC route developed rSBA titers >8, which was considered protective on the basis of recent population-based studies of meningococcal C conjugate vaccine efficacy in the United Kingdom (2,3). Therefore, CDC determined that this particular group of persons vaccinated by the SC route was sufficiently protected and that revaccination was not necessary. CDC cautions health-care providers to be aware that the licensed route of vaccine administration can vary among similar vaccines and recommends that providers carefully review and follow the route of administration indicated on the vaccine label and package insert before administering vaccines. This is especially important after introduction of a new vaccine product. Acknowledgments The findings in this report are based, in part, on contributions by the California Dept of Health Svcs; Illinois Dept of Health; Michigan Dept of Health; Pennsylvania Dept of Health; Kentucky Dept of Health; Vermont Dept of Health; MD Decker, MD, P Hosbach, PhD, G Gilmet, PhD, E Bassily, PhD, D Gordon, PhD, Sanofi Pasteur, Swiftwater, Pennsylvania; and W Atkinson, MD, National Center for Immunization and Respiratory Diseases (proposed), CDC. References
* As defined in 21 CFR 1240.62 (Postmarketing reporting of adverse experiences), available at http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?FR=600.80.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 9/20/2006 |
|||||||||
|