|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
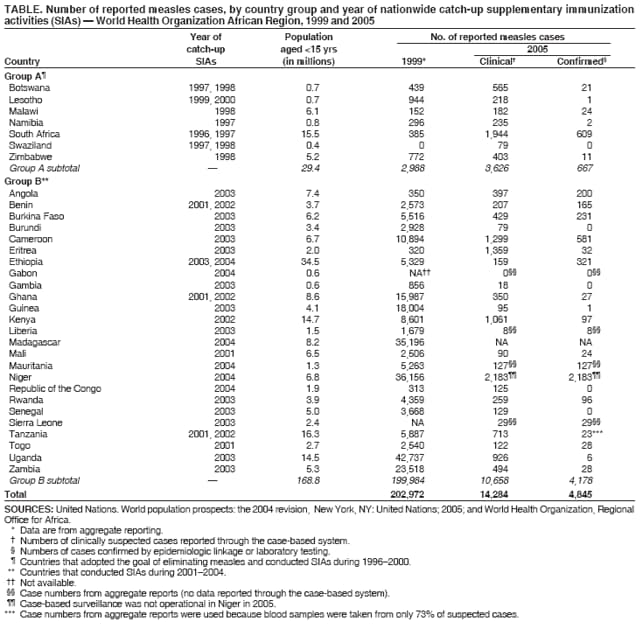
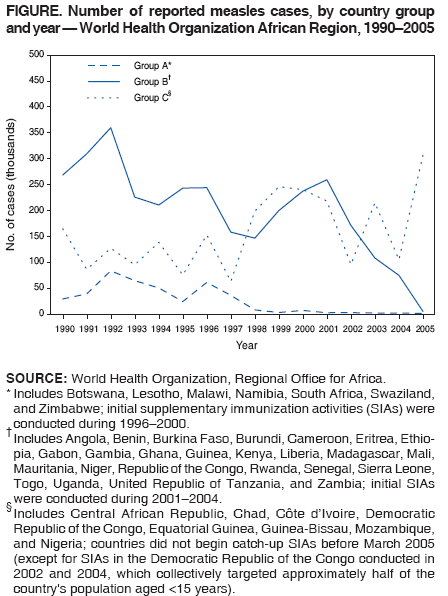
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Effects of Measles-Control Activities --- African Region, 1999--2005In 1999, of approximately 871,000 deaths from measles worldwide, 61% occurred in sub-Saharan Africa (1). In 2001, countries in the World Health Organization (WHO) African Region began an accelerated measles-control program to reduce by half by 2005 the number of deaths that were caused by measles in 1999 (2). The African Region accelerated measles-control program was based on four strategies: improving routine vaccinations; providing a second opportunity for measles vaccination through a routine, 2-dose vaccination schedule or through supplementary immunization activities (SIAs)*; improving measles case management; and establishing case-based surveillance with laboratory confirmation for all suspected measles cases. Seven countries in the region had already completed catch-up SIAs by 2000, before the regional program began; in 2001, additional countries in the region began implementing catch-up, and later, follow-up SIAs,† and steps were taken to improve routine vaccination coverage with measles vaccine and other vaccines in the Expanded Programme on Immunization schedule. This report summarizes the nationwide SIAs and other measles-control activities conducted in the WHO African Region during 1999--2004, analyzes the trends in reported measles cases since 1990, and compares the annual number of measles cases reported in 2005 with those reported in 1999.§ Immunization ActivitiesWHO and UNICEF publish annual country-specific estimates of routine measles vaccination coverage; these estimates are based on reviews of vaccination coverage surveys, national reports, administrative coverage data, and consultation with regional and local experts (3). According to these estimates, coverage with 1 dose of measles vaccine in the African Region among children aged 12--23 months increased from 52% in 1999 to 67% in 2004. In 2004, 37 of the region's 46 countries were estimated to have coverage rates >60%, and 17 countries were estimated to have coverage rates >80% (4). By 2000, seven countries in the African Region had completed national catch-up SIAs, and during December 2001--December 2004, 25 additional countries completed national catch-up SIAs. Ten of these 32 completed national follow-up SIAs. Measles vaccination coverage rates during these SIAs were >90%, except for the catch-up SIAs in Republic of the Congo (78%), Eritrea (82%), Ethiopia (87%), and Gabon (80%) and the follow-up SIAs in Lesotho (75%), Swaziland (81%), and Zimbabwe (85%). By December 2004, a total of 207.9 million children in 32 countries had been targeted by catch-up SIAs, which is 69% of the population of children aged <15 years in the African Region. During the same period, 16.1 million children aged 9--59 months in 10 countries were targeted by follow-up SIAs, which represents 14% of the population of children aged <5 years in the African Region. Measles SurveillanceSince the 1980s, the annual number of country-specific measles cases has been reported by the country's ministry of health each year to WHO's Regional Office for Africa. Before implementing catch-up SIAs, all countries reported measles cases to WHO through routine infectious disease information systems that provided aggregated data. The cases reported through this surveillance system were not laboratory confirmed; they were reported on the basis of clinical suspicion. After conducting their catch-up SIAs, countries began implementing a case-based surveillance system with laboratory confirmation of suspected measles cases. In this system, each case is reported using an individual case-report form, and a blood specimen is obtained for measles immunoglobulin M (IgM) testing at a national laboratory. When a cluster of three or more cases from a health-facility catchment area has been confirmed, subsequent cases from that area are considered confirmed by epidemiologic linkage, and blood samples are not collected. The quality indicators used for the case-based surveillance system include the proportion of reported cases with a blood specimen (goal: 80% of cases not confirmed by epidemiologic linkage) and the proportion of districts reporting at least one suspected case with a blood specimen per year (goal: 80%). For Niger and Tanzania, the total number of cases with a blood specimen was <80% of the aggregate case total, so aggregate case totals were used for analysis. For all other countries, blood specimens were obtained for >90% of reported cases. Analysis of Surveillance DataCountries were grouped according to the year in which they conducted their catch-up SIAs; number of reported cases by country group and year during 1990--2005 were calculated (Figure). Of the Group A¶ countries, six completed catch-up SIAs by December 1999, and the seventh completed its catch-up activities by the end of 2000; these countries had a measles-elimination goal rather than a mortality-reduction goal (5). Group B** consisted of 25 countries that completed nationwide catch-up SIAs during December 2001--December 2004. Group C†† consisted of eight countries that did not begin catch-up SIAs before March 2005 (except for SIAs in the Democratic Republic of the Congo conducted in 2002 and 2004, which collectively targeted approximately half of the country's population aged <15 years). The number of reported measles cases in Group A and Group B countries, which have all completed their SIAs, began decreasing steadily as SIAs were conducted (Figure). No decline was evident in the Group C countries; not all areas have been covered by SIAs, and yearly fluctuations in the number of measles cases have been observed. In countries that completed SIAs, the total number of suspected measles cases decreased 93%, from 202,972 in 1999 to 14,284 (Table); 1999 was chosen as the year for comparison because it is the baseline year for the measles mortality-reduction goal, and the initial catch-up SIAs in all countries other than the Group A countries were conducted after 1999. The number of cases in 1999 was obtained from aggregated reports of cases that were diagnosed on the basis of clinical signs and symptoms; few of these cases have laboratory confirmation, and they include other diseases consistent with the clinical case definition of measles (e.g., rubella). In 2005, after establishment of case-based surveillance, cases were confirmed by a laboratory or through epidemiologic linkage; confirmed case totals were available for all countries except Gabon, Liberia, Mauritania, and Sierra Leone. In 2005, aggregate data also were used for Niger because case-based surveillance was not fully operational in the country. Tanzania reported 713 possible cases through the case-based system, but because blood samples were obtained from <80% of cases, aggregate data were used in the calculations. Countries with no report for 1999 (Gabon) or 2005 (Madagascar) were excluded from the calculations. To maintain consistency in the case definition, clinically suspected measles cases reported in 2005 (i.e., which include cases not counted later after they had negative IgM serology results) were used in the calculations. The 93% decrease during 1999--2005 in suspected cases demonstrated substantial progress in countries that have implemented accelerated measles-control activities. To minimize the effect of using a single year as a baseline for a disease with cyclic epidemics, reports of suspected cases in 2005 also were compared with the average number of cases that occurred during 3 years (1998--2000). When the 3-year average was used as a baseline (N = 200,683 cases), reported cases also decreased 93%. Reported by: D Nshimirimana, MD, BG Masresha, MD, T Maumbe, A Dosseh, PharmD, Measles Program, Regional Office for Africa, World Health Organization, Harare, Zimbabwe. Dept of Immunization, Vaccines, and Biologicals, World Health Organization, Geneva, Switzerland. Global Immunization Div, National Center for Immunization and Respiratory Diseases (proposed), CDC. Editorial Note:The results of this report indicate a consistent and marked decrease in the number of measles cases reported from the WHO African Region country groups that completed nationwide measles catch-up SIAs during 1996--2004. These countries have experienced a >90% reduction in clinical measles cases in 2005 compared with 1999. In contrast, the number of reported cases continued to vary widely by year in the group of countries that had not completed nationwide catch-up SIAs. Although countries do not report measles deaths to WHO, an analysis of country-level data from 13 countries in the African Region that completed nationwide catch-up SIAs during late 2001 to early 2002 documented that the percentage reduction in reported deaths from measles was similar to that for reported cases of measles (6). The use and analysis of surveillance data in this report suggest that case-based measles surveillance with laboratory confirmation in the African Region is providing useful information for monitoring program effects. The increase from 2,988 cases in 1999 to 3,626 cases in 2005 from countries in Group A (Table) is largely a result of the increase in cases reported from South Africa. For example, in 2000, South Africa reported 117 confirmed measles cases (5), compared with 609 in 2005. During 2003--2005, South Africa experienced a large, nationwide measles outbreak involving 1,676 confirmed cases, the result of measles importation from Mozambique and failure to vaccinate enough of the population to prevent endemic measles transmission. The data in this report are subject to at least two limitations. First, data from a single year were used to estimate changes in a disease that has cyclic epidemics. However, when the average number of reported cases that occurred during 1998--2000 (compared with 2005) was used instead of data from 1999 only (compared with 2005), the percentage reduction was similar. Second, the system used for reporting cases changed in most countries; in 1999, the countries used aggregated reporting of clinically diagnosed cases, but in 2005, most reported laboratory-confirmed cases. Therefore, numbers of suspected cases reported in 2005 were used to estimate the decrease in cases during 1999--2005, which might have led to an even greater decrease. In addition, although the case definition for suspected measles remained the same, the change from the aggregate (in 1999) to the case-based system (in 2005) of reporting might have resulted in underreporting (because of the additional tasks of individual case reports and blood samples) or overreporting (because of increased awareness of measles surveillance after SIAs). By December 2005, approximately 87% of the population aged <15 years (267.2 million children) in the countries in the African Region had been targeted by catch-up SIAs. In 2006, nationwide catch-up SIAs are focusing on the areas that have not yet been covered, including 29 million children in southern Nigeria and 7 million children in the Democratic Republic of the Congo. Successful control of measles in the African Region will depend on conducting high-quality campaigns (i.e., campaigns that achieve >95% coverage) in these areas. At the same time, countries should continue to improve their routine immunization services, maintain high coverage with follow-up SIAs every 3--5 years, improve measles case management, and monitor their success by using case-based surveillance with laboratory confirmation to control measles and reach the global goal of reducing measles mortality. References
* Initial, nationwide catch-up SIAs target all children of a particular age group (in this region, children aged 9 months--14 years), with the goal of eliminating susceptibility to measles in the general population. Periodic follow-up SIAs then target all children born since the last SIA; follow-up SIAs are generally conducted nationwide every 3--5 years and target children aged 9--59 months, with the goal of eliminating any measles susceptibility that has developed in recent birth cohorts and protecting children who did not respond to their first measles vaccination. † These activities were supported by the Measles Initiative. Founded in 2001, the Measles Initiative is a partnership formed to reduce measles mortality and is led by the American Red Cross, the United Nations Foundation, CDC, WHO, UNICEF, and the Canadian International Development Agency. The initiative supported implementation of high-quality measles SIAs during 2000--2004 for approximately 40 African countries. Additional information is available at http://www.measlesinitiative.org. § By convention, Algeria and the island nations of the Comoros, Mauritius, Sao Tome and Principe, and the Seychelles are not routinely included in analyses of data from the WHO African Region. ¶ Botswana, Lesotho, Malawi, Namibia, South Africa, Swaziland, and Zimbabwe. ** Angola, Benin, Burkina Faso, Burundi, Cameroon, Eritrea, Ethiopia, Gabon, Gambia, Ghana, Guinea, Kenya, Liberia, Madagascar, Mali, Mauritania, Niger, Republic of the Congo, Rwanda, Senegal, Sierra Leone, Togo, Uganda, Tanzania, and Zambia. †† Central African Republic, Chad, Côte d'Ivoire, Democratic Republic of the Congo, Equatorial Guinea, Guinea-Bissau, Mozambique, and Nigeria.
Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 9/20/2006 |
|||||||||
|