|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
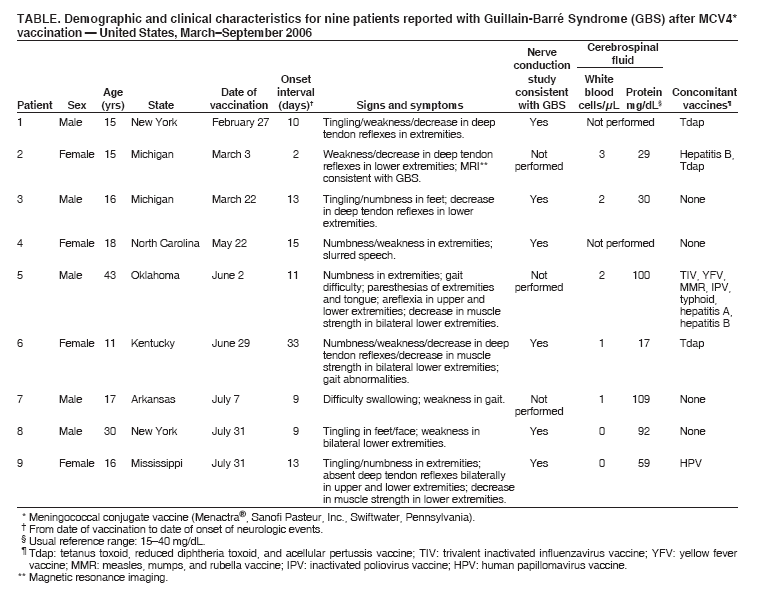
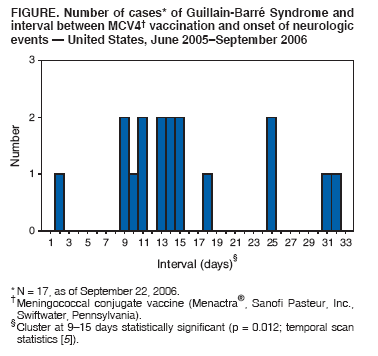
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Guillain-Barré Syndrome Among Recipients of Menactra® Meningococcal Conjugate Vaccine --- United States, June 2005--September 2006Please note: An erratum has been published for this article. To view the erratum, please click here.In October 2005, reports indicating a possible association between Guillain-Barré Syndrome (GBS) and receipt of meningococcal conjugate vaccine (MCV4) (Menactra®, Sanofi Pasteur, Inc., Swiftwater, Pennsylvania) were made to the Vaccine Adverse Event Reporting System (VAERS) (1). GBS is a serious neurologic disorder involving inflammatory demyelination of the peripheral nerves. During March 2005--February 2006, eight confirmed cases had occurred within 6 weeks (i.e., the time window of elevated risk noted for GBS after administration of other vaccines) after MCV4 vaccination (2,3). This report summarizes nine additional GBS cases reported to VAERS during March--September 2006. This report also provides a preliminary analysis of data from VAERS and the Vaccine Safety Datalink (VSD) since MCV4 became available in the United States in March 2005 and includes all 17 cases of GBS reported since June 2005. Although these data suggest a small increased risk for GBS after MCV4 vaccination, the inherent limitations of VAERS and the uncertainty regarding background incidence rates for GBS require that these findings be viewed with caution. Because of the risk for meningococcal disease and the associated morbidity and mortality, CDC continues to recommend routine vaccination with MCV4 for adolescents, college freshmen living in dormitories, and other populations at increased risk (4). Each of the nine most recent cases reported to VAERS was reviewed by a CDC medical officer and a clinical immunization safety assessment investigator from Boston University to confirm a diagnosis of GBS. Of the nine cases, eight met the surveillance case definition (KS Kohl, MD, The Brighton Collaboration, Atlanta, Georgia, personal communication, 2006), and one was a sensory variant of GBS diagnosed by the attending neurologist based on nerve conduction studies consistent with GBS. The following is an illustrative case report from the nine cases reported most recently (Table). Mississippi, July 2006On July 31, 2006, an adolescent girl aged 16 years from Mississippi received MCV4 and human papillomavirus (HPV) vaccines. On August 13, she experienced numbness and tingling in her extremities. On August 25, she was evaluated by a neurologist for increasing weakness and subsequently admitted to the hospital. On physical examination, she was found to have absent reflexes bilaterally in the upper and lower extremities and had decreased muscle strength in the lower extremities. Nerve conduction studies were consistent for GBS, and analysis of the cerebrospinal fluid showed the protein to be 59 mg/dL (reference range: 15--40 mg/dL) with no white blood cells. The patient received intravenous immunoglobulin, improved, and was discharged on September 5. As of September 7, she still had residual weakness but was continuing to improve. Case CharacteristicsClinical data for other possible causes of GBS frequently were not available when investigating the 17 cases of GBS after MCV4 vaccination. Campylobacter jejuni is a leading cause of gastroenteritis and the most frequent antecedent pathogen in GBS cases (5). None of the patients had reported diarrheal prodromes; however, many C. jejuni infections are asymptomatic. Three of the 17 patients had stool cultures; one was tested for C. jejuni, and the results were negative. A serum sample from one of the patients was tested for C. jejuni, and the result was negative; no other serum samples were available for testing. None of the states where the patients resided reported outbreaks of C. jejuni during June 2005--September 2006. The range of onset intervals (i.e., date of vaccination through date of onset of adverse event) for the 17 cases was 2--33 days, with a mean and median of 15.7 and 14 days, respectively (Figure). Using a temporal scan statistic, the cases were determined to be significantly clustered at onset intervals of 9--15 days and greater than expected by chance (p = 0.012 [6]). Comparison of RatesInformation from a managed-care organization within VSD indicates that approximately 94% of persons who have received MCV4 are aged 11--19 years (CDC, unpublished data, 2006). Therefore, analyses were limited to this age group and excluded two GBS cases in persons aged 30 years and 43 years. To assess whether the VAERS reporting rate for GBS after MCV4 vaccination was higher than expected, the VAERS reporting rate was calculated by dividing the 15 confirmed GBS cases in persons aged 11--19 years with onset within 6 weeks of vaccination by 7.46 million person-months (i.e., 5.39 million vaccine doses distributed to persons aged 11--19 years multiplied by 6 weeks follow-up per dose). The resulting rate was 0.20 per 100,000 person-months. The background incidence rate for GBS was estimated both from the Healthcare Cost and Utilization Project (HCUP), which is a multistate hospital discharge database, and the VSD database. Using 2000--2003 data from HCUP, the background incidence rate for GBS among persons aged 11--19 years was estimated at 0.11 per 100,000 person-months. Based on HCUP data, the ratio of the VAERS reporting rate of GBS after MCV4 vaccination to the background rate was 1.78 (95% confidence interval [CI] = 1.02--2.85). A separate analysis was performed, using a VSD background incidence rate of 0.11 per 100,000 person-months, based on 2000--2004 data and using a Poisson model to adjust for seasonal variation. Using these VSD data, the ratio of the VAERS reporting rate of GBS after MCV4 vaccination to the expected incidence rate was 1.77 (CI = 0.96--3.07). Finally, an analysis of MCV4 use based on VSD data revealed that, during March 2005--September 20, 2006, a total of 126,506 doses were delivered and no cases of GBS were observed among vaccine recipients aged 11--19 years within 6 weeks of vaccination (0.2 cases would be expected during that period). During the same period, two cases of GBS were reported among an equal number of persons aged 11--19 years from a matched comparison group receiving preventive care and who had not received MCV4 vaccination. Reported by: EJ Woo, MD, R Ball, MD, M Braun, MD, Center for Biologics Evaluation and Research, Food and Drug Admin, Rockville, Maryland. T Clark, MD, N Rosenstein Messonnier, MD, Div of Bacterial Diseases; M Wharton, MD, National Center for Immunization and Respiratory Diseases (proposed); C Vellozzi, MD, S Campbell, MSPH, E Weintraub, MPH, R Davis, MD, Immunization Safety Office, Office of the Chief Science Officer, CDC. Editorial Note:Neisseria meningitidis is a major cause of bacterial meningitis and sepsis in the United States. The case-fatality ratio for meningococcal disease is 10%--14% (4). Meningococcal disease also causes substantial morbidity; 11%--19% of survivors have sequelae (e.g., neurologic disability, limb loss, or hearing loss). Although rates of disease are highest among children aged <2 years, 62% of meningococcal disease cases in the United States occur among persons aged >11 years (4). During 1991--2002, the rate for persons aged 11--19 years was 1.2 per 100,000 per year and was higher than the rate for the general population. The Advisory Committee on Immunization Practices (ACIP) has recommended MCV4 vaccination for the prevention of invasive meningococcal disease (4). In October 2005 and April 2006, CDC and the Food and Drug Administration alerted health-care providers about a possible association between GBS and MCV4 (1,3). Since introduction of MCV4, a total of 15 cases of GBS have been reported in persons aged 11--19 years with onset within 6 weeks of MCV4 vaccination. The ratio calculated by using HCUP data, but not VSD data, to define the background incidence rate, suggests a statistically significant increased risk for GBS after vaccination with MCV4. The completeness of GBS reporting to VAERS, a passive surveillance system (7), is unknown. If underreporting to VAERS of GBS after MCV4 vaccination has occurred, the risk would be higher than estimated in this report. In addition, VSD has a limited ability to detect rare health events such as GBS; therefore, not finding any cases after vaccination in this population aged 11--19 years should not offer substantial reassurance regarding the safety of MCV4. Finally, the timing of onset of neurologic symptoms within 1--5 weeks of vaccination among reported cases continues to be of concern. Using the HCUP background incidence rate and assuming the ratio of 1.78 accurately represents the true magnitude of increased risk after MCV4 vaccination, the number of excess cases of GBS for every 1 million doses distributed to persons aged 11--19 years is approximately 1.25 (CI = 0.058--5.99). However, substantial uncertainty exists regarding the risk estimate, using either the HCUP or VSD background incidence rate. Furthermore, no surge in the frequency of GBS reports to VAERS was noted after either the October 2005 or April 2006 CDC reports, as might be expected if underreporting had occurred (e.g., after alerts for intussusception associated with RotaShield® vaccine [8]). GBS is a rare illness, regardless of etiology; expected incidence rates for GBS are not precisely known, and the available data cannot determine with certainty whether MCV4 increases the risk for GBS. Ongoing evaluation of GBS after MCV4 vaccination is being performed using VSD data. A larger study will be necessary to provide a more definitive assessment, but any such study likely will take several years to accumulate cases and attain sufficient statistical power. In May 2005, CDC recommended routine vaccination with MCV4 of adolescents, college freshmen living in dormitories, and others at high risk for meningococcal disease (4). However, CDC recommends that persons with a history of GBS not receive MCV4, although persons with a history of GBS at especially high risk for meningococcal disease (i.e., microbiologists routinely exposed to isolates of Neisseria meningitidis) might consider vaccination. Given the data in this report, ACIP will review the current recommendations for MCV4. A Vaccine Information Statement and fact sheet providing information on the vaccine and reported GBS cases is available at http://www.cdc.gov/nip/publications/vis/default.htm. An updated fact sheet for health-care workers on GBS and Menactra is available at http://www.cdc.gov/nip/vacsafe/concerns/gbs/menactra.htm. Because of the ongoing risk for meningococcal disease and the limitations of the data indicating a small risk for GBS after MCV4 vaccination, the additional cases reported here do not affect or change current CDC recommendations (4). CDC encourages all persons to report cases of GBS or any other clinically significant adverse events associated with MCV4 or any other vaccination to VAERS. Reports may be submitted securely online at http://www.vaers.hhs.gov or by fax at 877-721-0366. Reporting forms and additional information are available at telephone, 800-822-7967. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 10/19/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|