|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
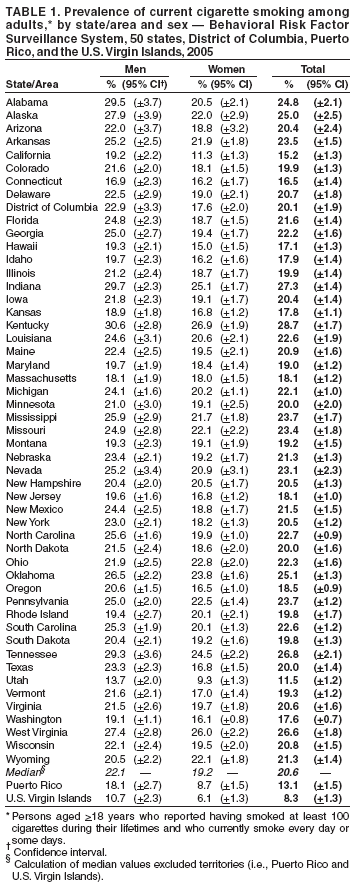
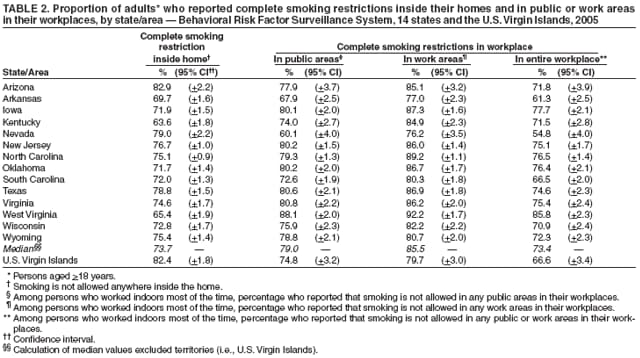
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. State-Specific Prevalence of Current Cigarette Smoking Among Adults and Secondhand Smoke Rules and Policies in Homes and Workplaces --- United States, 2005Smoking causes premature death and disease in children and adults who do not smoke but are exposed to secondhand smoke (SHS) (1). To assess the state-specific prevalence of current smoking among adults in the United States and the proportions of adults who report having smoke-free home rules* and smoke-free policies† in their workplace, CDC analyzed data from the 2005 Behavioral Risk Factor Surveillance System (BRFSS) (2). This report summarizes the results of that analysis, which indicated a threefold difference (from lowest to highest) in self-reported cigarette smoking prevalence in 50 states, the District of Columbia (DC), Puerto Rico (PR), and the U.S. Virgin Islands (USVI) (range: 8.3%--28.7%). Wide variations also were observed in USVI and the 14 states that assessed prevalence of smoke-free home rules (from 63.6% [Kentucky] to 82.9% [Arizona]) and smoke-free workplace policies (from 54.8% [Nevada] to 85.8% [West Virginia]). Evidence-based, comprehensive tobacco prevention and control programs that focus on decreasing smoking initiation, increasing smoking cessation, and establishing smoke-free workplaces, homes, and other venues should be continued and expanded to reduce smoking prevalence, exposure of nonsmokers to SHS, and smoking-related morbidity and mortality. BRFSS is a state-based, random-digit--dialed telephone health survey of the noninstitutionalized, U.S. civilian population aged >18 years. The 2005 BRFSS was conducted in 50 states, DC, PR, and USVI. The questions to assess SHS rules and policies were offered as an optional module and were used in 14 states and USVI. Estimates were weighted by age and sex distribution for each state/area population, and 95% confidence intervals were calculated. Because BRFSS data are state-specific, median prevalences rather than national averages are reported. The territories (PR and USVI) were excluded in the calculation of median prevalence. The median response rate among all states and DC was 51.1% (range: 34.6%--67.4%) (2). Respondents were asked, "Have you smoked at least 100 cigarettes in your entire life?" and "Do you now smoke cigarettes every day, some days, or not at all?" Current smokers were defined as those who reported having smoked at least 100 cigarettes during their lifetimes and who currently smoke every day or some days. To assess smoke-free home rules, respondents were asked, "Which statement best describes the rules about smoking inside your home?" The response options were 1) "Smoking is not allowed anywhere inside your home," 2) "Smoking is allowed in some places or at some times," 3) "Smoking is allowed anywhere inside your home," and 4) "There are no rules about smoking inside your home." To assess smoke-free workplace policies, persons who reported that they were employed and worked indoors most of the time were asked, "Which of the following best describes your place of work's official policy for indoor public or common areas, such as lobbies, rest rooms, and lunch rooms?" and "Which of the following best describes your place of work's official smoking policy for work areas?" Response options for the first question were 1) "Not allowed in any public areas," 2) "Allowed in some public areas," 3) "Allowed in all public areas," and 4) "No official policy." Response options for the second question were 1) "Not allowed in any work areas," 2) "Allowed in some work areas," 3) "Allowed in all work areas," and 4) "No official policy." Current Cigarette Smoking PrevalenceDuring 2005, the median adult smoking prevalence among all 50 states and DC was 20.6% (range: 11.5%--28.7%) (Table 1). Smoking prevalence was highest in Kentucky (28.7%), Indiana (27.3%), and Tennessee (26.8%) and was lowest in Utah (11.5%), California (15.2%), and Connecticut (16.5%). Smoking prevalence was 8.3% in USVI and 13.1% in PR. In the majority of states, men had a higher smoking prevalence (median: 22.1% [range: 13.7%--30.6%]) than women (median: 19.2% [range: 9.3%--26.9%]). Smoke-Free Policies in Homes and WorkplacesIn the 14 states that asked about smoking restrictions in homes and workplaces, the median percentage of persons who reported that smoking is not allowed anywhere inside their homes (i.e., complete smoke-free home rule) was 73.7%, and the median percentage of persons who worked mostly indoors and reported that smoking is not allowed in any indoor public areas or work areas within their workplaces (i.e., complete smoke-free workplace policy) was 73.4% (Table 2). In USVI, 82.4% of persons reported complete smoke-free home rules, and 66.6% reported complete smoke-free workplace policies. In all 14 states and USVI, respondents reported higher percentages of complete smoke-free policies in work areas (median: 85.5%§ [range: 76.2%--92.2%]) than in public areas of their workplaces (median: 79.0% [range: 60.1%--88.1%]). The states with the highest percentages of smoke-free home rules were Arizona (82.9%) and Nevada (79.0%); the states with the lowest percentages were Kentucky (63.6%) and West Virginia (65.4%). The states with the highest percentages of smoke-free workplace policies were West Virginia (85.8%) and Iowa (77.7%); Nevada (54.8%) and Arkansas (61.3%) had the lowest percentages. Reported by: E Maurice, MS, S Thorne, MPH, U Ajani, MBBS, A Malarcher PhD, R Merritt, MA, C Husten, MD, Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, Coordinating Center for Health Promotion, CDC. Editorial Note:Healthy People 2010 objectives call for reducing adult cigarette smoking prevalence to 12% (objective 27-1), reducing the proportion of nonsmokers exposed to SHS to 45% (objective 27-10), and increasing the proportion of workplaces and workers that are covered by smoke-free workplace policies to 100% (objective 27-12) (3). In 2005, Utah and USVI; women in Utah, California, and USVI; and men in USVI continued to meet the Healthy People 2010 objective for reducing adult smoking prevalence, as they did in 2004. Women in PR achieved the goal for the first time in 2005. Men in Utah met the goal in 2004 (11.7%) but not in 2005 (13.7%) (4). The present rate of decline in current smoking rates is not fast enough for most states to achieve the Healthy People 2010 objective of 12% (objective 27-1). Because the majority of SHS exposure among nonsmokers occurs in workplaces and homes, the only interventions that effectively protect nonsmokers from SHS exposure are legislation, policies, and rules that make workplaces and homes completely smoke-free (1). SHS exposure has decreased substantially during the past 20 years, in part because many employers and communities and certain states have implemented smoke-free policies and laws. As of March 1, 2006, six states (Delaware, Massachusetts, New Jersey, New York, Rhode Island, and Washington) had implemented laws (effective on or before June 1, 2006) that make private workplaces, restaurants, and bars smoke-free (5). In addition, several other states have implemented laws that make one or two of these three settings smoke-free. However, the findings in this report indicate that a substantial proportion of adults remain at risk for SHS exposure in their homes and workplaces because of lack of smoke-free rules and policies. Among the 14 states that used the optional SHS module, only Oklahoma has had statewide smoke-free laws for private workplaces since September 2003, but restaurants in Oklahoma were not included until March 1, 2006. The patterns of current smoking among U.S. adults might be beginning to mirror the current smoking patterns among middle and high school students, which have not changed substantially from 2002 to 2005; smoking prevalence rates in this student population have stabilized in the past few years (6). The lack of change in cigarette smoking might be attributed to the substantial increase in marketing expenditures by tobacco companies since 1998 and decreases in state funding for comprehensive tobacco-control programs since 2002 (7,8). In 2003, tobacco companies spent approximately $15.1 billion on advertising and promotion, which more than doubled these expenditures from 1998 (7). The Federal Trade Commission reported that price discounts paid to retailers or wholesalers to reduce the price of cigarettes to consumers accounted for $10.8 billion (71.4% of total advertising and promotional spending by tobacco companies in 2003) (7). In contrast, in the state fiscal year 2006, Colorado, Delaware, Maine, and Mississippi were the only states that funded their tobacco-control programs at the minimum levels recommended by CDC (8,9). The findings in this report are subject to at least four limitations. First, BRFSS does not sample persons in households without landline telephones, a population that might be more likely to smoke (2). In 2005, an estimated 94.2% of the U.S. population had telephones; however, noncoverage ranged from 2.1% of households in Connecticut to 10.0% of households in Arkansas and 23.8% in PR (2). Second, several states did not collect data for all 12 months of the year because of the severe hurricane season. Data from Mississippi and Louisiana only include information collected during January--August. PR did not collect data in March, and USVI did not collect data in July, October, and November. Third, estimates for cigarette smoking are based on self-report and are not validated by biochemical tests. However, self-reported data on current smoking status have been shown to have high validity (2). Finally, the median response rate was 51.1% (range: 34.6%--67.4%); however, the reliability and validity of BRFSS measures have been demonstrated (2). In the recently released report, the Surgeon General concluded that SHS causes premature death and disease in children and in adults who do not smoke (1). Children exposed to SHS are at increased risk for SIDS, acute respiratory infections, ear problems, and more severe asthma (1). The home is the place where children are most exposed to SHS, and children remain more heavily exposed to SHS than adults (1). Exposure of adults to SHS has immediate adverse effects on the cardiovascular system and causes coronary heart disease and lung cancer (1). The Surgeon General's report concludes that no risk-free level of SHS exposure exists (1). The report also concludes that eliminating smoking in indoor spaces fully protects nonsmokers from SHS exposure, whereas separating smokers from nonsmokers, cleaning the air, and ventilating buildings cannot eliminate this exposure (1). Laws and regulations that create smoke-free worksites and public places should be implemented to protect the health of the public. Everyone is encouraged to make their homes smoke-free to protect themselves and their families from exposure to SHS. Consumer education materials describing what the public, parents, and employers can do to make their environments smoke-free are available online at http://www.surgeongeneral.gov/library/secondhandsmoke/secondhandsmoke.pdf. Implementing smoke-free rules and policies in conjunction with other elements of a comprehensive tobacco-control program, such as increasing tobacco excise taxes, having sustained counter-marketing campaigns, expanding access to quitline services, and increasing insurance coverage for tobacco-use treatment (10), have been shown to increase cessation, decrease consumption, and decrease SHS exposure. Implementing comprehensive state tobacco-control programs that are funded at the minimum levels recommended by CDC (9) would accelerate progress in reducing tobacco use and SHS exposure. References
* Home smoke-free rules are private household rules that are adopted voluntarily by household members. They can include comprehensive rules that make homes smoke-free in all areas at all times and less comprehensive rules that restrict smoking to certain places or times (1). † Workplace smoke-free policies regarding smoking in public areas and work areas are established either by legislation (at the local or state level) or through smoke-free policies adopted voluntarily by employers. § Calculation of median values excluded USVI. Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 10/25/2006 |
|||||||||
|